

Post-Pandemic Excess Deaths in England
An Analysis of UK Deaths following Lockdowns & Covid Vaccinations, by John Sullivan & Steve Whitehouse, July 2022

1. Executive Summary
1.1 Key Findings & Objectives
In the last three months there has been a large surge in deaths in the UK, unrelated to Covid.
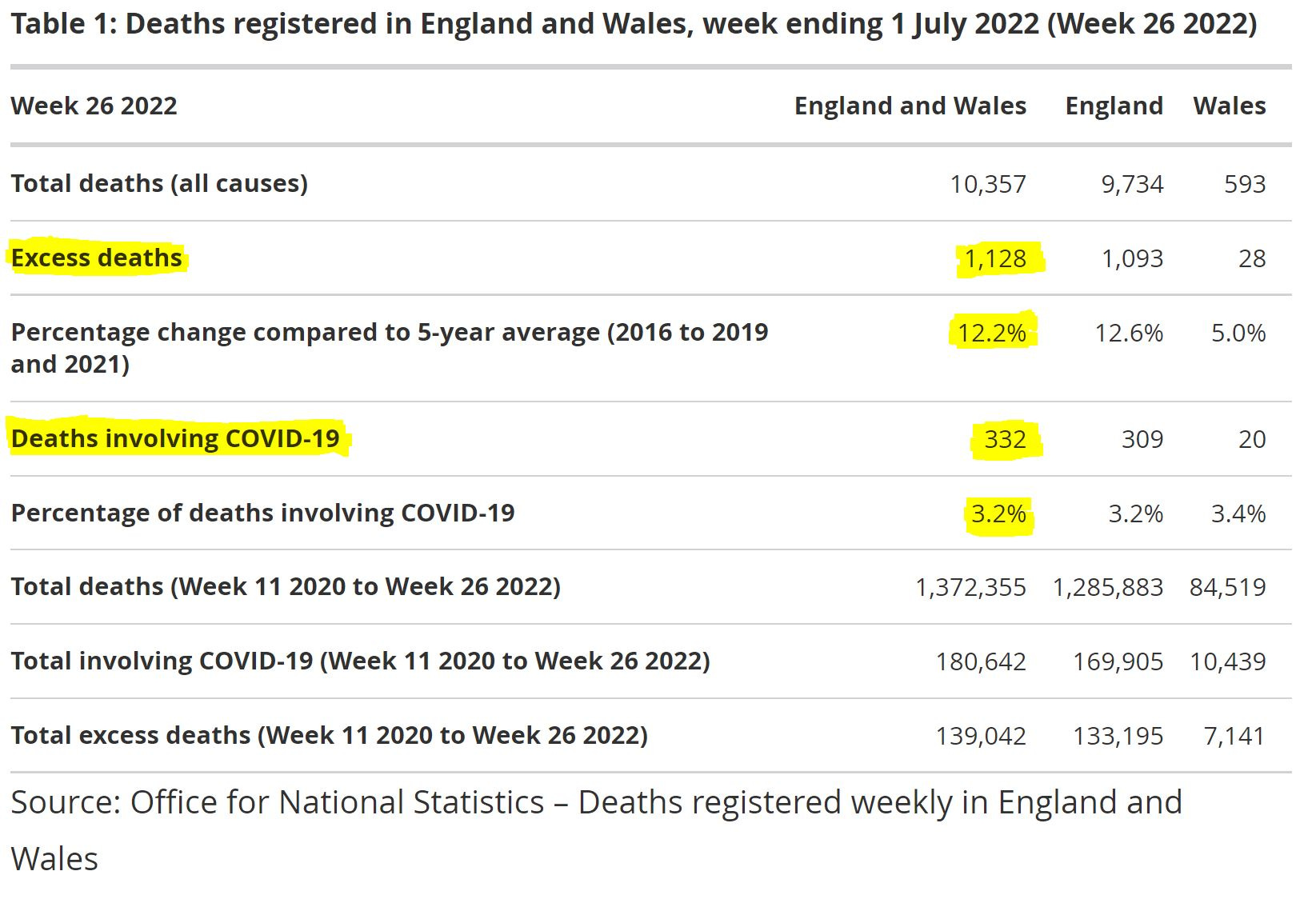
Following a trend which has now persisted for 10 weeks, the latest weekly report from the Office for National Statistics (ONS) - which we discuss in detail at section 4.2 - shows that there were 10,357 deaths in the week ending 1st July 2022, 1,128 or 12.2% above the 5 year average. Only 332 of these deaths “involve” Covid, with only 212 of those listing Covid as the underlying cause of death.
So there were 916 (1,128 - 212) more deaths than expected where the primary cause was not Covid, 796 (1,128 - 332) of which where Covid was not even a secondary factor. This brings the total number of these non-Covid excess deaths to something between 6,900 and 11,800 for the 10 week period from 23rd April to 1st July (see section 4.3 for details).
After 10 weeks, it is reasonable to conclude that this is not a temporary ‘blip’ in the numbers. Extrapolating to a full year (assuming things do not worsen further in Winter due to factors which may not yet be apparent), we can expect an annualised rate of up to 61,000 non-Covid excess deaths.
As detailed in section 4.2, the only plausible explanation for this very significant increase in excess deaths is that they are due to the lockdowns, the vaccines, or a combination of both.
In summary, the most significant of our conclusions - as detailed throughout sections 3 and 4 of this document - are as follows.
The worst of the pandemic was over by June 2020, and it had completely run its course as a significant public health threat by March 2021. Of the 90,000 excess deaths we estimate due to Covid, approximately 58,000 occurred during the initial outbreak and 32,000 during the following Winter. There have been very few deaths genuinely resulting from Covid since April 2021.
The empirical numerical evidence suggests there may have been up to 10,000 vaccine fatalities following the initial rollout to the most frail elderly population, during Winter 2020/21.
There have been up to 11,800 excess deaths in the past 9 weeks for which the ONS have reported (an annualised rate of 61,000 if it were to continue), which are not plausibly related to Covid.
In addition to the worrying rise in excess deaths in recent months, there are compelling reasons for concern about the impact of the initial vaccine rollout to the most frail elderly in the population, as detailed in section 3.3.
We therefore estimate a total of up to 22,000 deaths to date as a result of the lockdowns and/or the vaccines - but it is still early days as far as the manifestation of long term risks is concerned.
Our objective with this paper is to encourage an open and constructive dialogue around the true impact of the pandemic, especially on the elderly and vulnerable, as well as the impact of the interventions. Our key analysis approach is to use Excess Deaths data - which, prior to Covid, was the accepted key measure to assess the severity of a pandemic.
1.2 Situation Summary as at 15th July 2022
We show in section 4.1 that, while Omicron sub-variants are currently in widespread circulation across the UK, the number of people in mechanical ventilation beds in England was just 274 as at 14th July 2022 - around 1 in every 200,000 of the population, or 1 person in an area like the Metropolitan Borough of Gateshead.
Furthermore, the Intensive Care National Audit & Research Centre (ICNARC) reports an average of just 3 critical care admissions per day across England, Wales & NI for the 7 days to 30th June 2022.
There is currently no ‘deadly surge’ of Covid in the UK which represents any kind of serious public health threat and, as we show in section 3.2, there has not been one for well over a year. Most people currently in hospital “with the virus” are not there “because of Covid”. As most ordinary people now know for themselves, a bout of Omicron is generally no more debilitating than a mild cold.
1.3 The Official and Media Narrative
As we discussed in our very first Covid paper, the UK’s response to the initial outbreak ran counter to all previous scientific wisdom - from within the UK and internationally, including the WHO - on managing a pandemic. This set an inappropriate tone for the debate on how to proceed which continues to this day.
With some rare exceptions, including a brief article in the Daily Telegraph and recent publicity from Mark Steyn of GB News, news of these non-Covid deaths has been ignored by the MSM. Steyn has received both praise and criticism, from different sides of the debate, for highlighting that the MHRA “Yellow Card” reporting system currently contains over 2,000 reports of deaths of individuals in close proximity to receiving a Vaccine - 803 + 1,291 + 64 + 49 as per the following direct quote from the MHRA:
“The MHRA has received 803 UK reports of suspected ADRs to the COVID-19 Vaccine Pfizer/BioNTech in which the patient died shortly after vaccination, 1,291 reports for the COVID-19 Vaccine AstraZeneca, 64 for the COVID-19 Vaccine Moderna and 49 where the brand of vaccine was unspecified. The majority of these reports were in elderly people or people with underlying illness. Usage of the vaccines has increased over the course of the campaigns and as such, so has reporting of fatal events with a temporal association with vaccination. However, this does not mean that there is a link between vaccination and the fatalities reported. Review of specific fatal reports is provided in the summaries above. The pattern of reporting for all other fatal reports does not suggest the vaccines played a role in these deaths.”
The MHRA believe that these post-vaccine deaths represent ‘correlation, not causation’ and state, as above, that there is not a (causal) link. However, as we discuss throughout sections 3 and 4, there is substantial empirical and circumstantial data to challenge this conclusion.
Rather than acknowledge that the interventions to date may now be resulting in the harmful consequences which some dissenting voices warned of, there is currently a growing trend from many official and media quarters - including the UKHSA, the MHRA, the ONS, the NHS, the BBC, members of ‘independent Sage’ and others - to raise the level of alarm about a ‘potentially deadly surge’ in Omicron BA.4 and BA.5 “cases” and to encourage the public to accept another ‘booster’ shot of the (as we show in section 3.3) risky and ineffective vaccines.
We are concerned that calls for further winter restrictions (mask mandates, travel restrictions and lockdowns) will increase in stridency and gain irresistible momentum. David Nabarro of the WHO is now once again urging people to “prepare for winter lockdowns”. Commenting alongside Neil Ferguson on Bird Flu in 2005, Nabarro told the BBC that the “range of deaths could be anything between five and 150 million”. In the end, just a few hundred people died.
If our interpretations in this paper are correct, then it is entirely possible that any further ill-considered, panicked response measures will have a far greater ongoing impact - in terms of both overall deaths and continuing socio-economic damage - than the virus itself.
2. Background
2.1 About the Authors
This article contains independent research and analysis by the authors. We receive no external funding and have not benefited in any way from our work in challenging the official Covid narrative, either directly or indirectly.
We are Business Change, Project Management and Data professionals - in terms of education, a graduate engineer and PhD theoretical physicist. Our analysis in this paper is based on empirical numerical and circumstantial evidence, rather than any claim to specific medical expertise, and we leave it to others to explain the detailed medical reasons for what is so clearly apparent in the data.
Our sole objective is to expose the truth, as we adjudge it in our professional capacity - that official sources, the MSM and ‘big tech’ have wilfully and systematically misled the UK public about the danger from Covid19, and the harms from various poorly conceived interventions, since at least June 2020.
We will be submitting a copy of this analysis, along with our earlier paper “Covid-19 Deaths in England & Wales”, to the recently initiated public enquiry chaired by Baroness Heather Hallett.
2.2 Previous Work
In our earlier paper we analysed UK death statistics, from the start of the pandemic up to the date of publication in April 2021. We observed in that paper that the British public had been egregiously misled about the evolution of the pandemic, in terms of the evolving mortality, that the worst of the serious public health threat was already over by June 2020, and that the overall impact in terms of excess all-cause mortality had been exaggerated in the public consciousness.
Although we pointed out that excess “second wave” deaths during Winter 20/21 would not have been exclusively down to Covid, we could only discuss the potential for a future tsunami of lockdown deaths in the broadest hypothetical terms. In addition, we could only hint at the possibility of vaccine deaths, for two reasons:
We initially published that paper on LinkedIn. As many others have experienced over the past two years, a level of self-censorship was essential if we didn’t want it to be immediately removed and our accounts cancelled.
At the time, we could not be entirely confident ourselves that the supposedly “safe and effective” vaccines were not what the globalist public health propagandists, supported by their big tech and mainstream media collaborators, were telling us they were. There was certainly enough circumstantial evidence in the UK to raise significant doubt, but no ‘smoking gun’.
Some will no doubt assert that there is still no single smoking gun with regard to deaths - while the claims of 95% efficacy have been exposed as farcical, the situation re. vaccine injuries and deaths is not so easily assessed, especially given the ongoing lack of transparency around the data. However, as we shall show, the totality of the empirical and circumstantial evidence is compelling.
Here, we will provide our candid opinion of the non-Covid excess deaths in Winter 20/21, together with a frank assessment of the mortality statistics since then - we will call these ‘Post-Pandemic’ deaths, since we assert that the pandemic was over as a serious public health threat at the time of our earlier paper - i.e. by March 2021.
2.3 Why The UK Data Matters
The UK’s standing as an economic and military superpower has declined since the Second World War, but it still wields enormous influence around the world in terms of socio-political ‘Soft Power’.
While we have always had an ‘uneasy’ relationship with the EU, culminating in Brexit (which severely triggered the NWO globalists), our key involvement in other supranational institutions - the Commonwealth, NATO, the UN (and its agencies the IPCC & the WHO), the European Court of Human Rights (ECHR) and, last but not least the globalist World Economic Forum (WEF) - means that our influence on global socio-political culture far outweighs our hard power in economic and military strength.
Furthermore, and critically as far as the Covid pandemic is concerned, the UK continues to ‘punch above its weight’ in terms of (previously) globally-renowned educational institutions and selected industry sectors such as the Life Sciences.
Finally, the UK civil service and broader public sector, for all its latter-day faults as a ‘woke’ purveyor of Long March neo-Marxist dogma, does include some long-established administrative agencies - such as the ONS, the National Audit Office (NAO) and others - which provide professional, ‘independent’ analysis and data services. While far from perfect (we still do not have, after more than 2 years, a publicly accessible, consolidated database of pandemic statistics as we described in the very first paper in our Covid series) publicly available UK data relating to the pandemic has been and is among the best in the world.
So when the pandemic modelling of Neil Ferguson - who had been previously discredited on multiple occasions - was used to justify unprecedented lockdowns, aka house arrest for healthy, law-abiding citizens, it mattered and the consequences were global. When official UK data continues to be misrepresented, distorted, censored, cherry-picked, or otherwise obfuscated to further a partisan (globalist left-wing) political agenda, it matters and the consequences are global.
It is the socio-political influence described above which continues to mean that a false narrative around official UK data is used to justify further alarmist calls for mandated mask-wearing, a return to lockdown, vaccine coercion and all the other lunacy that has led to the global dystopia of the past two and a half years.
If the UK reintroduces mask mandates, lockdown restrictions and coerced ‘booster jabs’, the World will follow. The battle in the UK matters.
3. Review of Pandemic Deaths to April 2021
3.1 Consistency of UK Data Sets
As we noted in our previous paper, ‘comparing apples with apples’ is a constant challenge when collating the different publicly available data sets in the UK - there are a number of different government agencies and professional bodies reporting relevant data, but their reporting methods vary in terms of granularity (e.g. UK wide v. England and Wales only) and period end dates.
As time passes, this challenge becomes ever more difficult to reconcile, as the reporting protocols of individual bodies change and some agencies are reorganised or replaced by successors - as was the case for example when Public Health England (PHE) was superseded by the UK Health Security Agency (UKHSA). Recent changes to the official Covid ‘dashboard’ - produced by the UKHSA - mean for example that most statistics are now updated weekly rather than daily.
Since England and Wales account for a large majority - approximately 88% - of the UK population as a whole, we do not dwell too much here on the occasional switching between slightly different data sets, particularly as we would not claim accuracy of better than 12% for the more speculative of our hypotheses.
3.2 Summary Analysis of Deaths
As we described in our earlier paper, England and Wales suffered ~111,000 excess deaths from the start of the pandemic up to the end of March 2021; ~58,000 in Spring 2020 and a further ~53,000 during the winter of 2020/21. When combined with the peak rates of excess deaths, it was clear that the “winter resurgence” was nowhere near as severe as the initial pandemic outbreak. Figure 1 below is reproduced from the earlier paper for ease of reference.
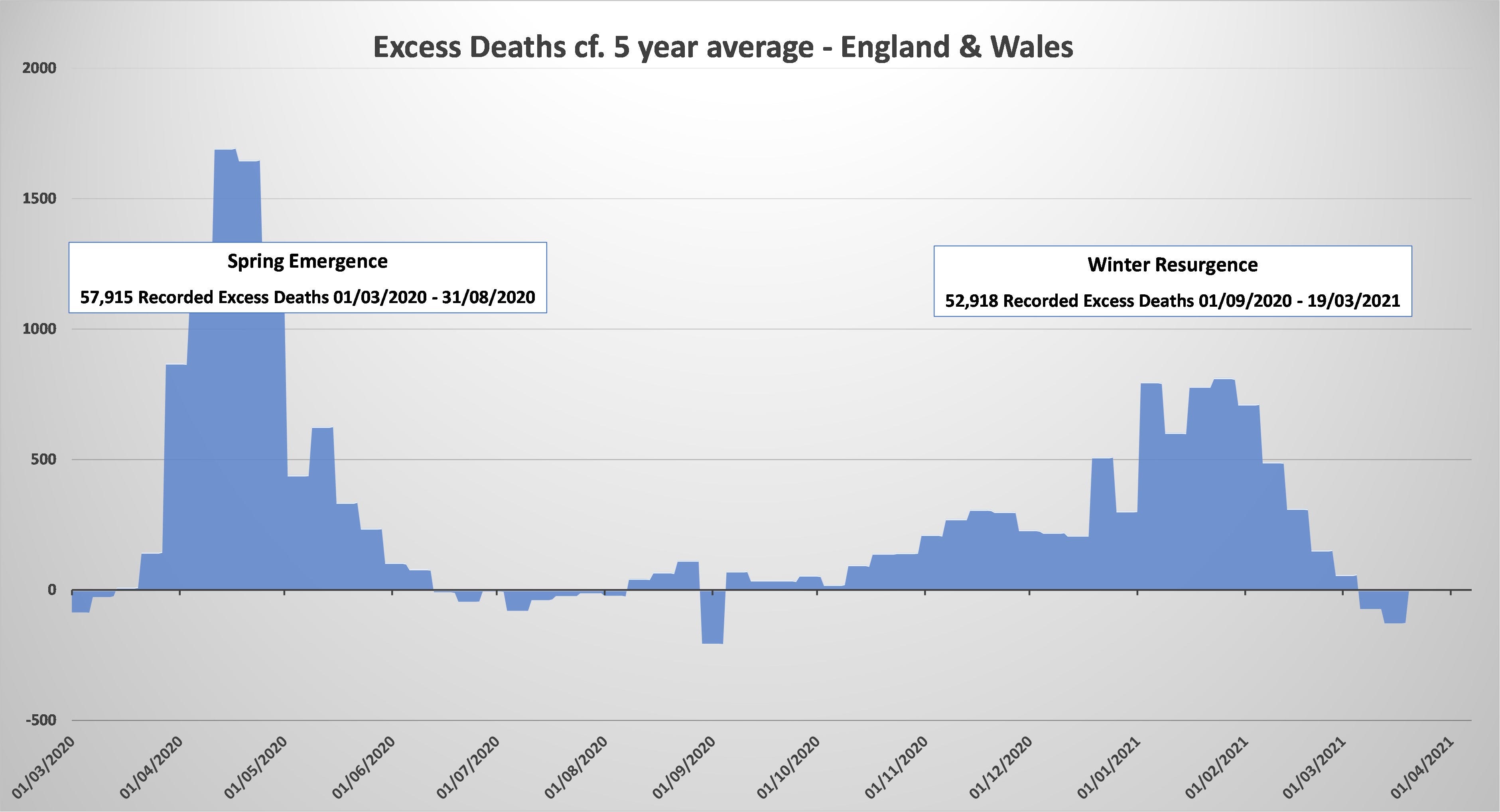
At the time of publication of our previous paper, excess deaths had started to go negative (see March 2021 in above chart). This trend continued for several months in total, with 17 weeks of an 18 week period in Spring and early Summer 2021 having a below average number of total deaths.
In total during the period to 2nd July 2021, there was a deficit of ~6,000 ‘all cause mortality’ deaths compared to the 5 year average, the most plausible and obvious reason for which is that many of the “Covid related” deaths in Winter 20/21 were amongst the frail elderly who did not have long to live - many of these people would have died during the next few months in any event. It is not unreasonable to consider these early deaths when considering the genuine overall effect of the pandemic; if they are properly taken into account, the overall excess mortality of the “second wave” reduces from ~53k to ~47k.
We previously hypothesised that some of the excess deaths would have been due to undiagnosed, untreated or aggravated conditions resulting from the lockdowns. Given the lack of hard data, it is impossible to accurately quantify such an effect, but an increase of just 1% in the usual annual death toll in England and Wales would have meant over 5,000 lockdown-related deaths - with a corresponding reduction in excess deaths attributable to Covid: Our running total of ~47k for the “second wave” would then reduce further to ~42k (compared, remember, to ~58K for the initial outbreak in Spring 2020 - although, as can be seen from the above chart, there was also a small number of ‘negative excess deaths’ in Summer 2020).
Although there are some esoteric details of this analysis which can be debated, it has always been clear and undeniable that the “second wave” was significantly less deadly than the initial outbreak.
But now we must consider the impact of the lockdowns and vaccines during Winter 2020/21 - were they ‘wise and miraculous interventions’ which reduced the impact of the “second wave” as seen in the data? Or may they actually have caused more problems than they solved - even on the narrow criteria of death statistics, i.e. ignoring all other socio-economic impacts?
We’ve already mooted above the potential negative impact of lockdowns on non-Covid death numbers - albeit that we can only speculate very broadly in the absence of high quality, publicly available data. Lockdown proponents though would (and do) claim that lockdowns, by ‘slowing the spread’, saved many thousands (even millions) of deaths from Covid itself - which would far outweigh any collateral damage from non-Covid lockdown deaths. There has always been precious little evidence for such claims by the lockdown enthusiasts. However, we now have empirical evidence that their alarmist fearmongering was based on false and exaggerated claims.
In December 2021, the UK’s Chief Medical Officer Chris Whitty - whose behaviour throughout the entire pandemic and post-pandemic period has, to put it mildly, lacked an appropriate level of professional detachment - told us that ‘everything we know about Omicron is bad’. It was clear at the time to any independent analyst that this was blatantly false, and it has become ever more obvious in the months since - during which time, Whitty has mysteriously disappeared from public view. There can only be one conclusion; Whitty outright lied.
It is beyond dispute that Omicron is a much milder version of the virus than the original ‘Wuhan strain’ of the original outbreak. However, in Winter 20/21 it was the ‘Kent’ (later re-designated as ‘Alpha’) variant which was prevalent in the UK. How deadly, in truth, was Alpha? We now have irrefutable proof that Chris Whitty (and others) were prepared to state bald untruths in order to further their alarmist lockdown and vaccine coercion agendas. It would be a foolish person who believes that they were being transparently truthful in Winter 20/21 - let’s look at the empirical evidence, of which there is now more than sufficient.
The virus has continually mutated from the original deadly Wuhan strain to milder, but more transmissible variants. Today, huge numbers of people in the UK are carrying sub-variants of Omicron but, crucially, very few people are seriously ill or dying. The Alpha variant was an early step in that evolution and, while it was not as mild as Omicron, neither was it credibly as bad as the original strain. There is no compelling evidence that the UK lockdowns of Winter 20/21 - which, it should not be forgotten, went entirely counter to all previously agreed pandemic planning criteria - were either necessary or effective in '“preventing 10’s or 100’s of thousands of Covid hospitalisations and deaths”.
But what about the vaccines?
As we described in the earlier paper, the vaccines did not plausibly arrive in time to significantly reduce the number of deaths in winter 20/21 - as even the UK Prime Minister conceded at the time.
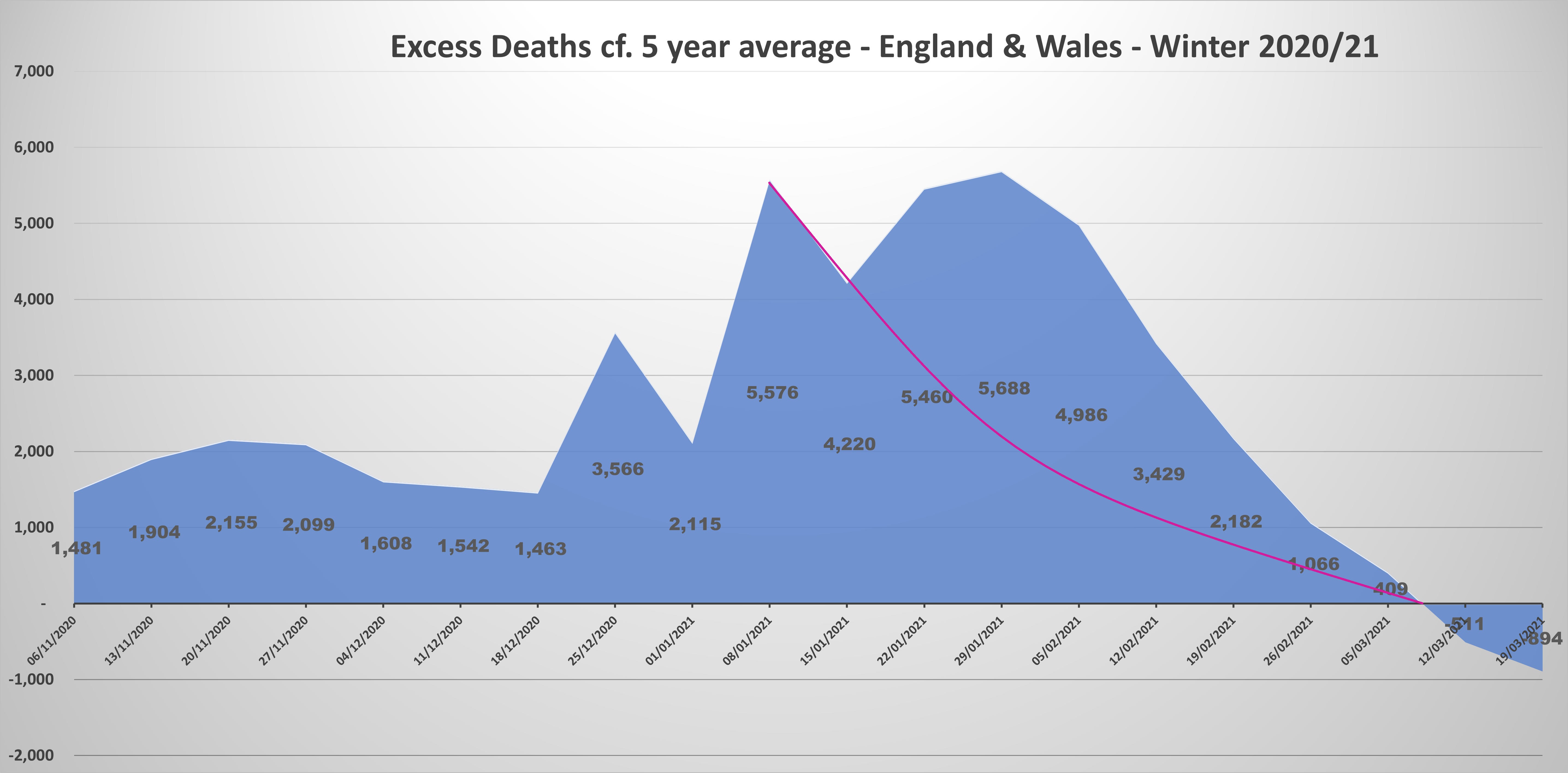
Let’s take a closer look at the death profile in January 2021, by zooming in on the chart from figure 1 and considering the deaths at weekly granularity.

Rates of excess mortality rose until the first week in January 2021 and, apart from a marked decline in the second week of the month, held steady throughout January. They then began a steady decline from the first week of February.
This levelling off of the excess death rate, from the start of January, was far too soon for the vaccines to have been a factor, given that the first vaccine was not administered in the UK until 8th December 2020, and that the vaccines are reported to need 3 weeks to build immunity; indeed, “cases” and deaths within 21 days of vaccination are counted in unvaccinated statistics.
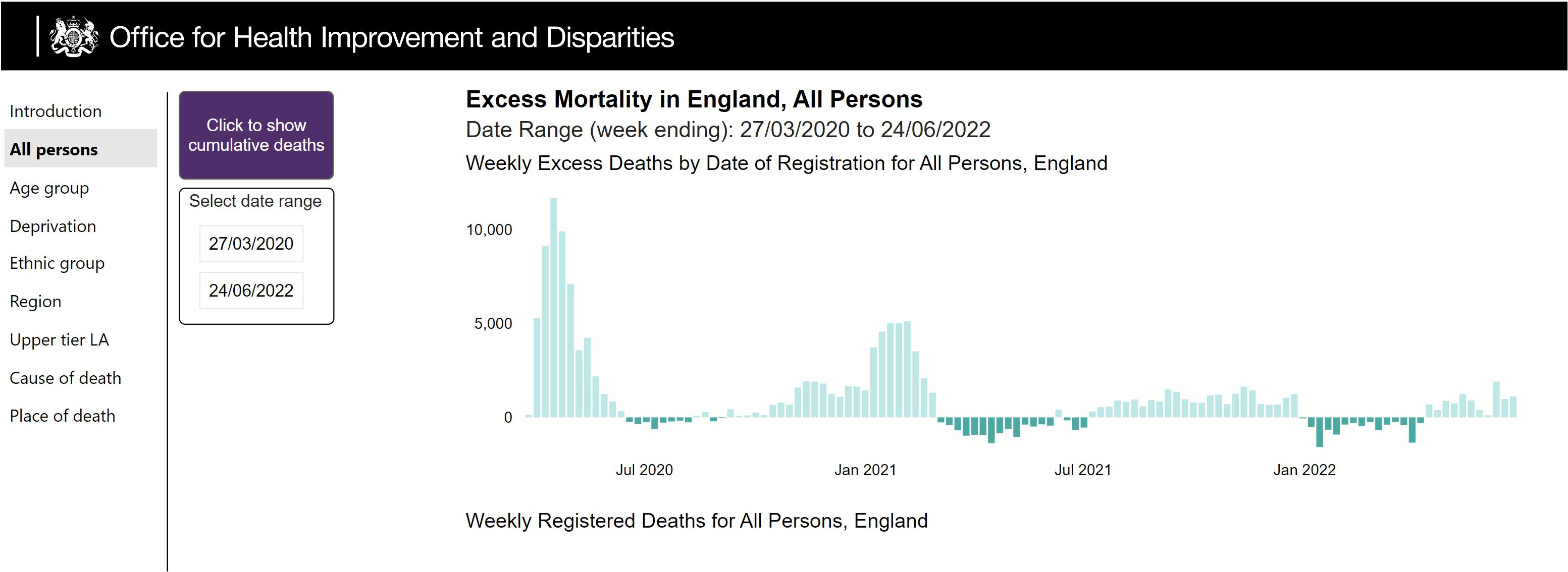
It is notable that reported “Covid deaths” peaked a few weeks later than excess deaths, as per figure 4 (reproduced from our earlier paper).
As we explained in the earlier paper, many of these “Covid deaths” (over 8,500 in England & Wales for January 2021 alone) were not caused by Covid, but were misattributed deaths from other causes. The apparent peak in deaths around 23rd January was a simple artefact of the peak in “cases” (positive test results) on January 1st - anyone dying within 28 days of a positive test result was recorded as a “Covid death”, irrespective of the true cause.

The 7 day average of “cases” peaked on 1st January 2020, exactly concurrent with the levelling off of excess deaths, before the brief drop in the second week of January. How to explain this scenario, given the well-publicised and intuitive delay of several weeks between infection and death? As with so much of the data, the evidence is circumstantial, but we can postulate a plausible hypothesis, as follows.
The initial peak in deaths at the start of January, before a brief one-week decline, is consistent with the Kent/Alpha strain being somewhat less deadly - deaths up to the end of 2020 would have been almost exclusively due to the earlier strain; once Alpha took hold, excess (Covid) deaths began to reduce.
But deaths immediately rose again the following week, plateaued for a week or two and then fell dramatically. Why?
3.3 Potential Short-Term Vaccine Deaths
How many vaccine deaths may have resulted from the initial rollout to the eldest and frailest of our population?
The data clearly shows that the rise in excess deaths stalled at the start of January, at exactly the same time as the rise in “cases” - so falling “cases” were clearly not the reason. Given the short timescales, this could also not have been due to the vaccines, nor to the post-Christmas lockdowns. Ergo, there must have been another factor at play - the most likely candidate being a reduction in the fatality rate from the Kent/Alpha variant which became prevalent in the UK during December 2020.
Exactly as we saw with Omicron a year later, Covid “cases” rose but deaths fell, due to a more transmissible but less fatal variant. This is consistent with everything else we’ve seen since the initial outbreak in Spring 2020.
Yet excess deaths remained elevated throughout January. Again, there is an obvious explanation once Covid itself, due to lack of compelling evidence, is properly discounted as ‘prime suspect’. Given the lack of fully transparent data during the initial rollout, we will never know for sure how many of the most vulnerable population may have been fatally injured by the vaccines, but we can dispassionately examine the available circumstantial evidence.
The first vaccine was administered in the UK on 8th December 2020, when a significant rise in “cases” provided fertile breeding ground for alarmist fearmongering from ‘public health experts’, inducing panic amongst the general population and a general clamour to receive the ‘miracle jabs’.
The original vaccine trials reported “mild or moderate” immediate reactions to the vaccines, such as fevers, headaches and diarrhoea for more than 1 in 10 of the trial participants, per the quotes below from the UK Medicines and Healthcare products Regulatory Agency (MHRA).

While these “mild or moderate” reactions may have been harmless enough to the mostly young, healthy volunteers in the initial trials, they could plausibly have been far more deadly to the frail elderly - especially those isolated in care homes under lockdown conditions, many of whom would have also been sadly afflicted with dementia to some degree. The original trials were not focussed on this most at risk cohort, and were vague with regard to the age profile of each study group as per, for example, the Pfizer protocol document for the original clinical trials:
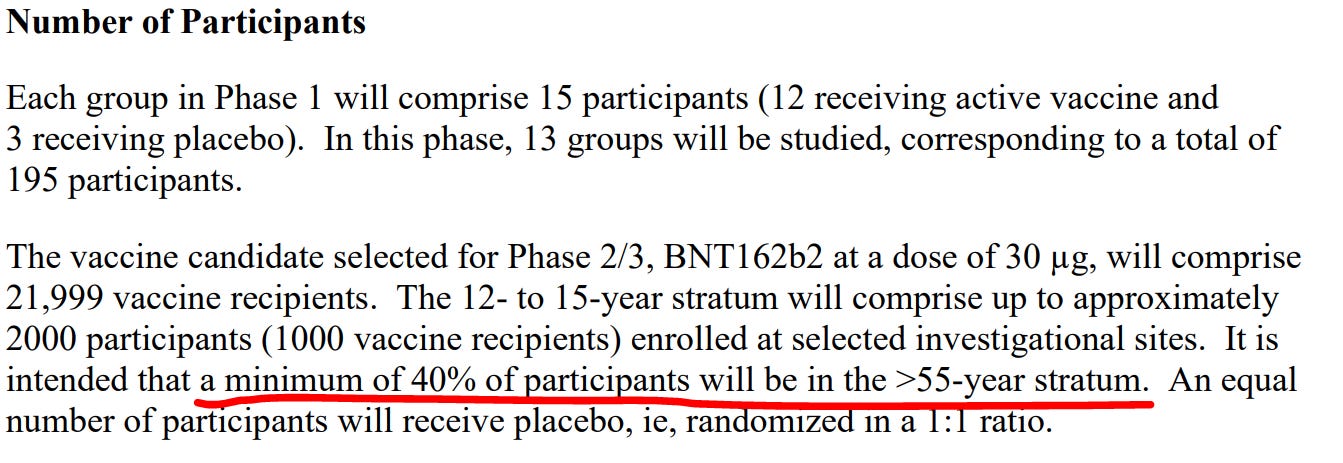


Disregarding for a moment what we now know about the true efficacy of the vaccines, there was never any convincing proof, before the rollout began, that the vaccines would be safe for the frail elderly cohort to whom they were initially administered. Indeed, given what we always knew about “mild or moderate” reactions from the initial trials, it stretches credibility that the vaccines would not have resulted in the deaths of significant numbers of this population.
Any quantitative estimate of likely vaccine deaths during January 2021 must necessarily be speculative. Figure 8, based on figure 3 above, provides an illustration of what the excess death curve may have looked like if the drop in the first week of the month did indeed represent the start of a reducing trend in deaths from the mutated virus itself; we reiterate - this would have been entirely consistent with a virus which was evolving to become less fatal as it became more transmissible.
However, the illustration at figure 8 excludes consideration of any positive effect from vaccines as the rollout progressed - it is not unreasonable to argue that excess deaths would have remained somewhat elevated through February and March, had the vaccines not been administered to a significant proportion of the population by then.
With a paucity of hard data, we’ll never know to what extent this would have been the case, but our subsequent experience with Omicron, as well as the undeniable peak in mortality rates during the initial outbreak, makes it extremely improbable that the ongoing evolution of the virus into ever more transmissible, ever less deadly strains would - at any stage - have led to an increase in overall mortality rates. We can therefore look at November and early December 2019 as the absolute worst case scenario for deaths without the vaccine in early 2021.
Taking all of these complex factors into account, we suggest that the vaccines may have been responsible for up to one third of the excess deaths during January and February 2021:
In late 2020 and early 2021, around 10,000 deaths may have been caused by the vaccines in England and Wales alone.
As reflected at figure 1, there were approximately 53k excess deaths during the winter of 2021, to the time of publication of our previous article. Other than the clear and obvious misattribution of deaths, we were circumspect about the impact of lockdown and vaccine-related deaths. With the passage of time and the continuous emergence of confirmatory evidence, we can now be confident that true Covid deaths during the “second wave” must be adjusted as follows:
Deaths caused by the impact of lockdowns - a 1% increase equates to 5,300 deaths.
Deaths where Covid was a factor, but death was sadly ‘due’ anyway within a few months - the chart at figure 2 reveals a period of negative excess mortality in Q2 2021, with an aggregate shortfall of around 6,000 deaths.
Up to 10,000 deaths among the frail elderly which were directly due to the vaccines.
In aggregate, these adjustments reduce the estimated overall impact of the “second wave” from ~53k to ~32k excess deaths due to Covid (rather than to our panicked and ill-judged response). Combining this number with the ~58k deaths during the initial outbreak, we arrive at an assessment of total Covid mortality throughout the pandemic of ~90k (as per our analysis in section 4, we do not consider that there has been any significant number of genuine Covid fatalities during the period since April 2021).
4. Recent Rise in non-Covid UK Excess Deaths
4.1 Covid Situation Review
The ONS estimate that, UK wide, there were ~3.5m Omicron infections as of week ending 6th July 2022) - so there is no question that the virus is in widespread circulation.
However, the number of people in mechanical ventilation beds in England, as at 14th July 2022, was just 274 (Gov.UK) and the latest weekly report from ICNARC, shows an average of just 3 Covid patients per day were admitted to critical care across England, Wales & NI for the 7 days to 30th June 2022.

There is currently no ‘deadly surge’ of Covid in England which represents any kind of serious public health threat and, as we show in section 3.2, there has not been one for well over a year. Most people currently in hospital “with the virus” are not there “because of Covid”. As most ordinary people now know for themselves, a bout of Omicron is generally no more debilitating than a mild cold.
4.2 The Red Flag in Recent Data
In section 3.2, we considered the potential short term adverse impact of the vaccines, with respect to the most vulnerable elderly population who received the initial doses.
There has also been much speculation in various quarters with regard to potential long term safety concerns - the potential for myocarditis and pericarditis for example, as well as possible effects on human fertility.
The ONS publish a weekly analysis of deaths in England and Wales (data for Scotland and Northern Ireland is reported separately as the ONS has no jurisdiction in these devolved nations). The latest ONS report, published on 14th July 2022 and covering the week ending 1st July, shows that deaths for that week were 1,128 (12.2%) above the 5 year average for the same week, while there were just 332 deaths “involving Covid” (only 212 of which recorded Covid as the underlying cause of death).
Taking Covid out of the equation completely, including cases where it was a secondary or contributing factor, there were 796 unexplained excess deaths in a single week.
So what is the likely cause of these excess deaths? In principle there are 4 possibilities:
Additional deaths from illnesses such as cancer and ischaemic heart disease which went untreated during the pandemic.
Long-term complications following Covid which were not identified by the doctor certifying the death.
Deaths caused directly or indirectly by the widespread rollout of the Covid vaccines.
Other, e.g. an undetected epidemic of some other disease or a random variation from the norm.
Options 2 and 4 are implausible and not statistically credible. The chances of doctors across the country failing to identify long term complications from Covid for example, after more than two years of non-stop Covid and ‘Long Covid’ propaganda, is close to zero. By the same token, a random variation from the norm of this magnitude would be improbable enough in isolation - statistically close to impossible, for a summer week with no public holiday - but a significant increase in excess mortality has been evident in the figures for many weeks now.
The only plausible explanation for this very significant increase in excess deaths is that they are due to the lockdowns, the vaccines, or a combination of both.
4.3 Analysis of Excess & Reported “Covid” Deaths in 2022
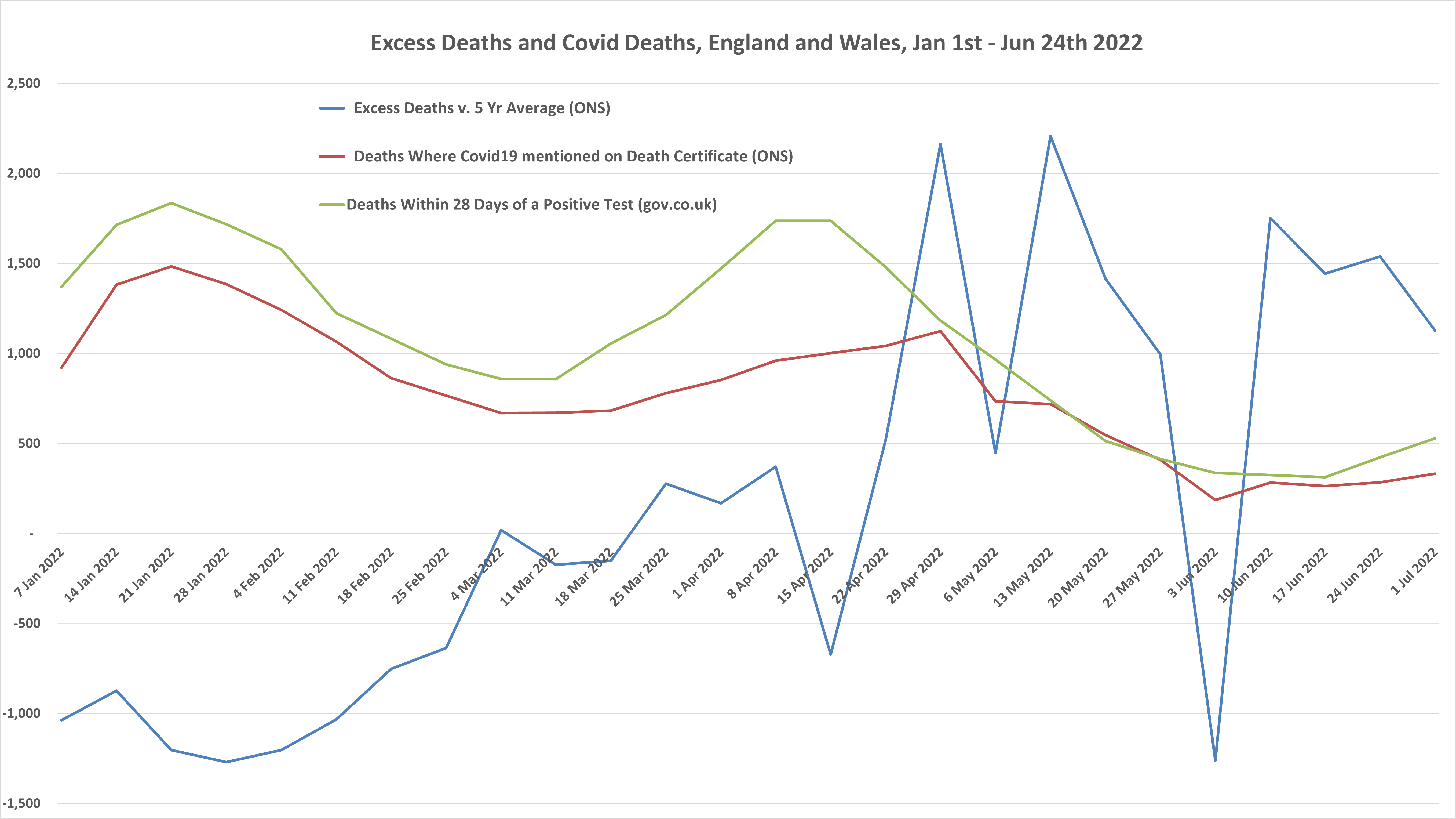
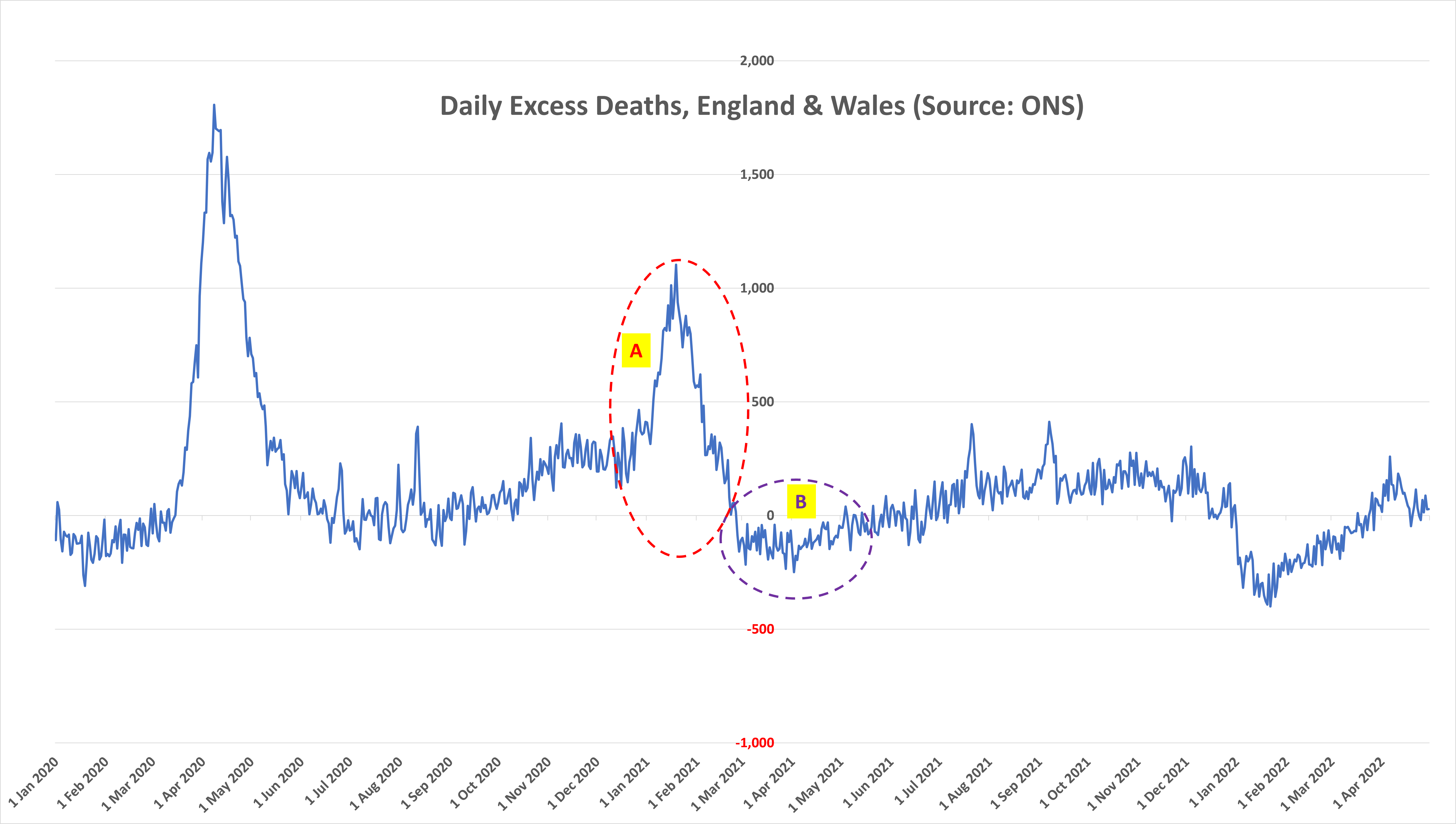
In 2022 up to 22nd April, there was a net deficit of nearly 8k deaths, compared to the 5 year average. This can be explained by the inclusion of 2021 numbers in the 5 year average (2016-19, and 2021) - while the “second wave” was far less severe than has been officially hyped, as we have explained, there was nevertheless a significant number of excess deaths in January and February 2021 (see ringed area ‘A’ at figure 12 below) which distort the 5 year average during Q1.
The rise in reported “Covid deaths” during April - in terms of both death certificate registrations (red line) and deaths within 28 days of a positive test - is entirely consistent with the rise in “Cases” during April. However, the lack of accompanying excess deaths during this period reinforces once again that these were vanishingly unlikely to be genuine Covid deaths - especially given that the 5 year average is distorted in the other direction by the negative excess death rate during this period in 2021 (ringed area ‘B’ at figure 12).
In total, during the early part of 2022 to 22nd April, there were 23,412 more reported “Covid deaths”, based on Death certificate registrations which mentioned Covid19, than excess deaths. This is consistent with what we have seen throughout the pandemic, whereby deaths with ‘incidental’ Covid infections have wrongly been attributed (or interpreted as due) to Covid.
To any impartial observer, it could not be more obvious that almost no one has been dying from the Omicron variant during 2022.
Since April 22nd however, the headline situation has reversed; the fall in reported “Covid deaths” (following a fall in “cases” a month or so earlier) is directly at odds with the rise in excess deaths. Between 23rd April and 24th June, excess deaths total ~11,800 compared to ~4,900 “Covid deaths”, the vast majority of which, as we have already argued, are not actually due to Covid. Crucially, from late May through June 2021, excess deaths were very close to the 5 year average - so we would expect no distortion to the 2022 comparison.
We are thus left with anywhere between 6,900 (11,800 - 4,900) and 11,800 ‘unexplained’ excess deaths, in a period of just 10 weeks. This, were it to continue, would equate to an annualised rate of up to 61,000 excess deaths, which can only plausibly be due to either the impact of lockdown on undiagnosed/untreated conditions, or vaccine-induced fatalities.
This is surely worthy of a formal investigation by the authorities and/or the mainstream media, or inclusion in the recently initiated public enquiry chaired by Baroness Hallett?
We would be more than happy to offer our services to assist with such an investigation, and will be submitting a copy of this analysis to the public enquiry.
5. Conclusions
On one side of the Covid ‘debate’, lockdown and vaccine proponents claim (retrospectively, as the original justification was only to “flatten the curve”) lockdowns saved countless lives and that vaccines too have saved up to 20 million lives globally to date.
At the other extreme, certain parties claim that the vaccines are killing “hundreds of thousands” in the UK alone, based on misinterpreting and/or misrepresenting cherry picked data - for example by not factoring a robust understanding of age stratification effects in vaccinated populations, and not sanity checking their conclusions with actual deaths data.
To some extent, the mistakes of the latter group are understandable, given that we have all been fed a continuous litany of half-truths and outright lies from official and ‘expert’ sources during the pandemic. More moderate dissenting voices bemoaning the madness of mask mandates, house arrest and vaccine coercion for entire populations, have been ruthlessly trolled and censored.
However the behaviour of the professional Covid alarmists is unforgiveable, and criminal, in our view. While amateur individuals and organisations can be forgiven for occasionally getting things wrong, it is clear beyond doubt that many in ‘public health’, Big Tech, Big Pharma, the MSM and others have wilfully misled the public and repeatedly violated the principle of informed consent.
We acknowledge that some details of our own hypotheses are somewhat speculative and we are open, as ever, to constructive criticism. We are certain, however, that the ‘official’ narrative is a complete misrepresentation of the facts.
In summary, we conclude that:
The total number of deaths ‘from Covid’ has been ~90,000, making Covid far more comparable, in population adjusted terms, to Asian Flu in the 1950's than Spanish Flu at the end of the First World War.
~58,000 of these deaths occurred in Spring 2020, during the initial outbreak.
The remaining ~32,000 deaths were spread through the winter of 2020/21.
The worst of the pandemic was over by June 2020 and the true pandemic was completely over as a significant public health threat by March 2021. The inescapable implication is that the entire array of ‘non pharmaceutical interventions’ (NPI’s) was futile and completely unnecessary.
The common perception that the vaccines saved hundreds of thousands, or even tens of thousands, of lives in the UK is completely unsupported by the empirical evidence. Following the initial outbreak in Spring 2020, the virus was set on an evolving path to ever more transmissible - but, crucially, ever milder - strains which, together with increasing natural immunity from exposure, meant that the pandemic was always going to wane rapidly as a serious public health threat. Like the NPI's, the rush to vaccinate was futile at best.
Up to 10,000 vaccine fatalities may have resulted from the initial rollout amongst the frail elderly.
We have seen up to 12,000 non-Covid excess deaths in a recent 10 week period, which can only plausibly be attributed to the NPI’s and/or the vaccines.
Finally, the jury is still out on the long term health consequences of the NPI's (before we even begin to consider their socio-economic damage) and the repeat vaccination of most of the population.
There are many voices in the medical community and elsewhere who cautioned against the folly of imprisoning healthy people and effectively shutting down healthcare for months at a time, and too the rush to rollout novel vaccine technology indiscriminately across all age groups and risk profiles. We can only hope that the dissenting voices of so many health professionals - who would, in normal times, be protected as whistle blowers, but have instead been widely censored, professionally defamed and denounced as crackpots - will be proven over-pessimistic with time.
If, on the other hand, their warnings prove to be even partially borne out, the criminal negligence and deception we have highlighted here would be just the start of an overwhelming human catastrophe.
Disclaimer of Liability ™
Whilst we endeavor to make our products toxic (1,291 side effects), we make no representations or warranties of any kind, express or implied about their efficacy and safety.
We cannot guarantee that your gene 144 won’t be deleted, your X / Y Chromosome won’t be inverted, your gene 69-70 won’t be deleted or mutated, that you may experience loss-of-function due to protein folding, that your gene E1, E3, E4 won’t be deleted, that you won’t receive shots full of magnetic graphene oxides, nano-biosensors and self-integrated bio-circuits (motherboards, transistors, routers, antennas, etc…).
We do not guarantee that you won’t be MAC Addressed as per Clown Schwab’s instructions (COVID -19 is a rare but narrow window of opportunity to rethink, reinvent, reset our world), that your Cancer Fighting CD8 T Cells won’t be suppressed.
By using our products you agree that you automatically become legally a trans-human and therefore our property since you are GM-modified using our patented mRNAs (CERTIORARI 12–398).
Trans-humans do not enjoy any human or other rights of a state and this applies worldwide. Our patents are under US jurisdiction and law, where they were registered.
Any reliance you place on our products is therefore strictly at your own risk.
We care,
CEOs Murderna & Schizer.
...
Dr. Red Pill Fact Checker: They make sh$t!
Schizer (1minute video)
https://librti.com/page/view-video?id=1438
Murderna (1minute video)
https://librti.com/page/view-video?id=1515
Micro-Tech in COMIRNATY Quackcine – New Zealand D SOS
https://nzdsos.com/wp-content/uploads/2022/04/Presentation-Microtech.pdf
How to Detect your MAC Address (e.g: “Pfizer borg 00:00:5e:00:53:af”)
https://forbiddenknowledgetv.net/are-you-or-someone-around-you-chipped-how-to-find-out/
Micro-Tech Patents (50) – Charles Lieber – Caught!
https://drtrozzi.org/2021/12/30/nanotech-expert-charles-lieber-first-high-level-covid-criminal-convicted/
Covid-19 Quackcines Worldwide Democide - 1,291 Side Effects – Schizer Approval Document Reveals
https://childrenshealthdefense.org/wp-content/uploads/pfizer-doc-5.3.6-postmarketing-experience.pdf#page=30
Suppression of Cancer Fighting CD8 T Cells - 100% of People Tested pre and post Covid-injections.
https://drtrozzi.org/2022/04/06/global-cancer-rates-exploding-post-vaccines-being-covered-up/
Safe and Effective: 16 German and Austrian Mayors Under 60 Are 'Suddenly and Unexpectedly' Dropping Dead.
https://rairfoundation.com/epidemic-german-and-austrian-mayors-under-60-aresuddenly-and-unexpectedly-dropping-dead/
Schizer Massive Data Fraud: Time to Lock them all Up!
https://drtrozzi.org/2022/04/29/time-to-lock-them-up/
How Bad is my Batch?
https://howbadismybatch.com/
The Covid Lies of the Century
https://doctors4covidethics.org/wp-content/uploads/2022/04/The-Covid-Lies-updated.pdf
Murderna Quackcine Patented 9 Months Before Plandemic on 2019-03-28
https://www.veteranstoday.com/2022/04/11/moderna-vaccine-patented-9-months-before-pandemic-thanks-to-the-fauci-baric-manmade-sars-viruses/
Covid-19 Plandemic Blueprint – RKM Lockstep 2010 Report.
https://themillenniumreport.com/2020/07/rockefeller-lockstep-2010-was-blueprint-for-2020-covid-19-pandemic/
Event 201, a High-level Pandemic Exercise on October 18, 2019, in New York
https://www.centerforhealthsecurity.org/event201/
50 Efficacy Studies that Rebuke Vaccine Mandates
https://brownstone.org/articles/16-studies-on-vaccine-efficacy/
United States D.O.D issued a contract for ‘COVID-19 Research’ in Ukraine 3 months before COVID-19 officially existed
https://expose-news.com/2022/05/18/us-dod-covid-research-contract-nov-2019/
Ten different surveys all show the vaccines are not "safe and effective" -- not even close
https://stevekirsch.substack.com/p/eight-different-surveys-all-show?utm_source=email&s=r
Dr David Martin | Covid Terrorism, Murder, and Racketeering
https://drtrozzi.org/2022/05/28/dr-david-martin-covid-terrorism-murder-and-racketeering/
We declare government and medical agencies must be held accountable!
https://globalcovidsummit.org/news/declaration-iv-restore-scientific-integrity
Planned Worldwide Infanticides
https://palexander.substack.com/p/warning-fda-cdc-nih-moderna-and-pfizer?s=r
'Blow-up Pandemic Mortuary' Set up in 2019 - UK
https://francesleader.substack.com/p/covid-truth-by-uk-funeral-director?s=r
EXCLUSIVE: Shocking microscopy photos of blood clots extracted from those who “suddenly died” – crystalline structures, nanowires, chalky particles and fibrous structures
https://www.naturalnews.com/2022-06-12-blood-clots-microscopy-suddenly-died.html
Graphene COVID Kill Shots: Let the Evidence Speak for Itself
https://www.globalresearch.ca/graphene-covid-kill-shots-let-evidence-speak-itself/5763418
Dr. Ryan Cole: COVID Vaccines Are Producing Unusual And Surprising Numbers Of Cancers
https://rumble.com/v15plmb-dr.-ryan-cole-covid-vaccines-are-producing-unusual-and-surprising-numbers-o.html
The "safe and effective" narrative is falling apart
https://stevekirsch.substack.com/p/the-safe-and-effective-narrative
"The Elites are Planning to Kill Billions of People" -- Prime Minister of Malaysia (2015)
https://twitter.com/cryptowala65/status/1546003810253803521
Boris Johnson's Father Wants to Reduce Britain’s Population to Around "10 or 15 million" by 2025. (2012)
https://twitter.com/FBNHistory/status/1547685928042278915?utm_source=substack&utm_medium=email