

Pandemic Preparedness in the UK

This article was first published on LinkedIn in late February 2021. Since both authors have since ‘parted company’ with that site, it is now re-posted here. We have resisted any temptation to update it in the light of developments over the past 20 months, since the vast majority of our points remain painfully relevant - vaccine safety & efficacy, as well as China emerging ‘relatively unscathed’, notwithstanding.
Summary
This article examines the preparation by the UK government for dealing with a pandemic disease outbreak. We address a number of items:
How the UK prepared for a pandemic disease.
How we should have prepared.
The impact of inadequate preparation.
Urgent lessons, before next winter as a minimum.
Under item 1, we review the UK strategic planning activities as reflected in key published documents.
On point 2, we set out a view of what good preparation would look like, in terms of strategic / detailed planning and, crucially, the advance actions that would have been essential to establish the foundations of an effective real-time response.
We compare our expectations of 'good preparation' to the actual strategic planning activities and conclude that the strategic planning approach was fundamentally flawed. The lack of adequate preparation had profound negative effects on our national response from the outset, continuing to this day. We discuss a number of the most severe impacts under item 3.
Item 4 is the critical one for any review process. Reviewing historical failings is futile unless real lessons are learned and changes implemented. Sadly, it is clear from the government's 'roadmap out of lockdown' that no such lessons have yet been learned; claims of 'following the data' are asserted - and accepted by inept politicians and media - despite all evidence being to the contrary.
But lessons can still be learned for the medium and longer term. We must prepare properly for any resurgence or new virus next winter, especially in terms of NHS surge capacity and infection control in hospitals and care homes. We must never again allow a lack of preparation by the NHS to be a reason for tolerating unproven and damaging national lockdowns.
We must also use the lessons learned from this traumatic national experience to expedite the creation of a written constitution, which is now so clearly needed to save this country from future such dystopian episodes.
Background
Discussion of the Covid19 pandemic, more than any other public health event in history, has dominated UK public and private discourse for the past 12 months - hardly surprising given the devastating effect of both the death toll and the collateral impact of draconian restrictions on so many aspects of normal life in our previously liberal democracy.
But there has been depressingly little genuine scrutiny, analysis or debate about either the preparation or the real-time response. The agenda has been utterly dominated by a one-sided, emotionally disingenuous narrative - that extreme and unconstitutional restrictions are necessary to prevent an even more catastrophic toll from a deadly virus which "doesn't discriminate".
Whatever else may be up for debate, it is absolutely undeniable that the impact of the virus is discriminatory. It disproportionately affects the elderly, those with existing health and obesity issues, and those unfortunate enough to be 'looked after' in hospitals and residential care facilities. Claims by the Health Secretary to have built a “protective ring around care homes” are particularly hollow, given the belated action which amounted to little more than attempting to close the stable door after the horse had bolted. Care home residents were imprisoned but not protected.
The UK response has failed to protect our vulnerable elderly, failed to prevent shocking levels of hospital-acquired (nosocomial) infection, and the socio-economic consequences have been disastrous. The 'cure' has been nothing of the sort, and massively worse than the disease - not that you'd know this from the constant propaganda put out by our political class and main broadcast media channels. The motivations for such an unbalanced narrative are varied; covering of tracks, vested financial interests, political agendas and more, but it is the ruthless censorship of dissenting voices which is perhaps most concerning.
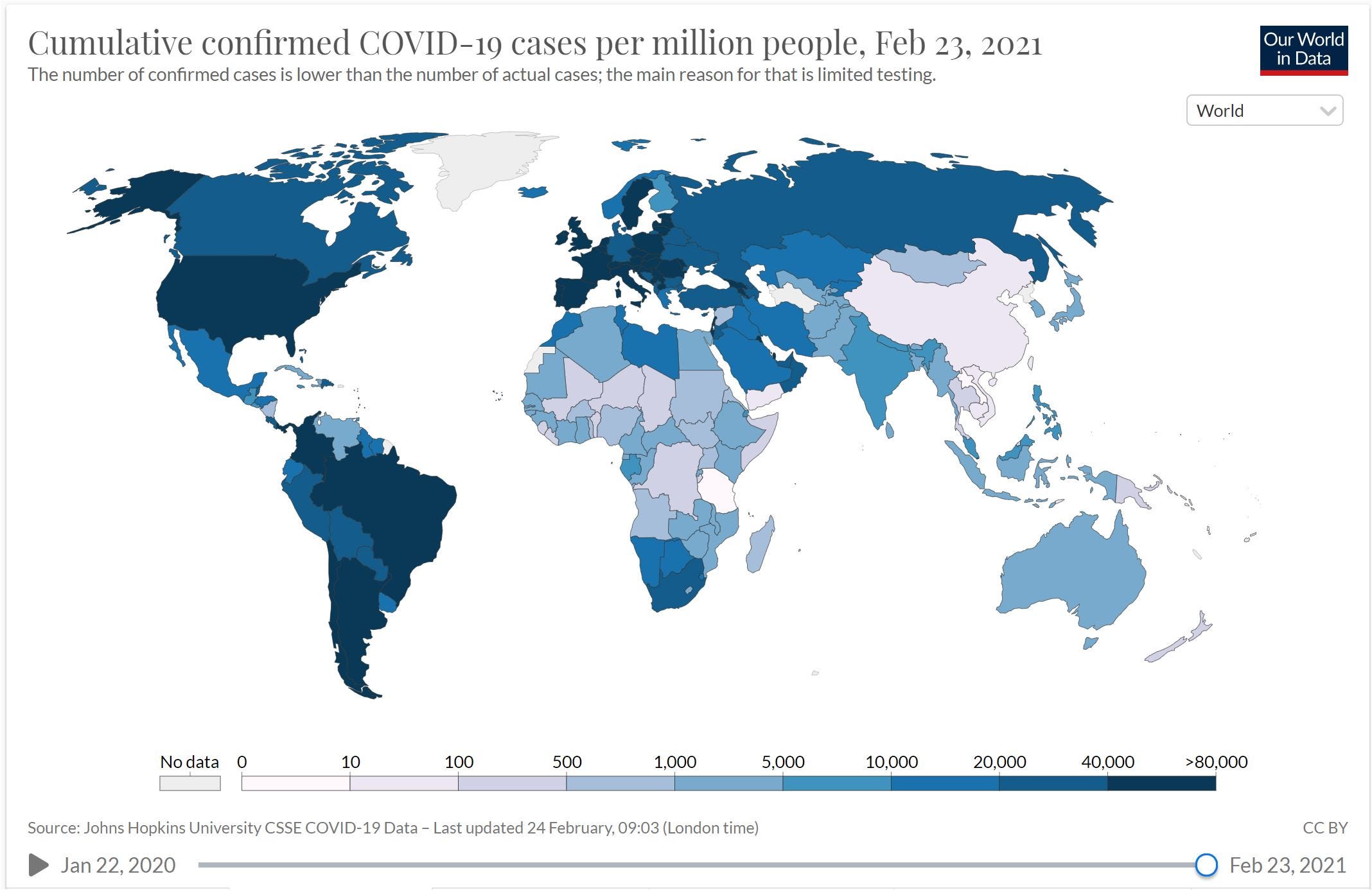
While the global scale of the pandemic in historical terms is far from clear at this point, and is likely to remain so for some time yet, the variation in levels of sickness and death across different countries and regions is huge. The reasons for this are debated, as is the likely longevity of each 'success story'. Comparisons abound - between East and West, Sweden & the rest of Europe, Florida and California, Australasia and everywhere else.
The progress of some developing regions is a particular enigma: Is the apparent 'light' toll in much of Africa an artefact of a lack of monitoring & reporting, population demographics (younger people), relative lack of obesity, vitamin D levels, other? Why has India, with 20 times the population of the UK, seemingly had only 3 times the cumulative number of cases (12m v. 4m)?
The debate is massively compounded by factors beyond the immediate toll in terms of sickness and death; the collateral impact of so-called 'non-pharmaceutical interventions' to 'control' viral spread - socio-economic, mental health, non-Covid deaths and so on.
Regardless of detail, it is beyond dispute that the impact of the pandemic and/or the response in the UK has been devastating. To date (Feb 2021); well over 100,000 excess deaths compared to 5 year average levels (a huge number of these in elderly care homes and many others resulting from nosocomial infection), the largest economic contraction in 300 years, the education and development of a generation of youth hugely disrupted, the possibility of an ongoing mental health crisis, extreme curtailment of basic civil liberties, and more.
It is equally clear that alternative approaches were available. Sweden did not impose unconstitutional lockdown measures and achieved better health outcomes without violating the basic human rights of its citizens.
The unprecedented psychological war conducted by the British Government against its own people continues to be a particularly pernicious and shameful aspect of this sorry episode, especially given the openly far-left agenda driving some of the individuals on the SAGE SPI-B sub-committee, aided and abetted by the BBC and other mainstream media outlets.
The serendipitous fact that many of the lockdown measures support the more extreme climate alarmist agenda should also ring serious alarm bells for anyone who values freedom and truly being guided by rational science. Curtailment of the aviation industry, restricting travel in general, and control of people's private lives all represent a potential 'softening up' process for future draconian impositions.
It is critical we do not now concede that "there was no other way". Culpable politicians and technocrats need to be held accountable, not just for their manifest failings but also for willfully misleading the country.
So what should we have done differently, and what should we do better in future?
UK Government Preparations
One of the criticisms sometimes levelled at the UK Government's response to the crisis is that they jettisoned a "perfectly adequate" pandemic response plan in favour of a panicked reaction triggered by scenes of Armageddon from communist China and Lombardy.
Another is that the results from Exercise Cygnus, a 2016 trial designed to test our pandemic preparedness based on a theoretical severe outbreak of H2N2 'flu, were not acted upon.
But are these claims true or are they, like so much else in this woeful episode, evolving into unchallenged urban myths? Did the UK ever have a coherent, detailed and workable pandemic response plan, or do the issues with our post-facto response stem primarily from a complete failure of preparation?
A detailed review of strategy and planning documents published by (agencies of) the UK government is contained in the Appendix. We provide a brief summary in this section.
One constant throughout the documents is the frequent assertion that a pandemic was one of top threats to the UK, if not the top threat; this pandemic came as no surprise to those responsible for dealing with the response. But published strategies and plans were inadequate, outdated (ranging from 2011 to 2014), and not sufficiently scenario-based. The only scenario to have seemingly influenced UK preparations was the mild impact of the 2009 H1N1 outbreak. Lessons (mis-)learned from that event led to complacency and the ongoing national disaster in which we are still embroiled.
There has been some discussion in the media about the Exercise Cygnus 'war games', conducted by PHE in 2016. Results from the Exercise Cygnus were not used to update the main documents, indeed full details have not been made public though some redacted information is available, which might have been written by Sir Humphrey Appleby. This gem for example:
“LESSON IDENTIFIED 1: Organisations should ensure that their Emergency Preparedness Resilience and Response training and exercising is consistent with best practice”
This 2017 video record of an NHS England Board discussion of emergency preparedness and response - including learnings from Exercise Cygnus - reveals just how seriously those at the top of the NHS took their responsibilities towards "one of top threats to the UK". But at least, in the words of the chair, they "took assurance".
Our focus in this article is on the UK preparation and response, but a brief mention of the World Health Organisation, WHO, role is merited. This 91 page document from October 2019, with contributions from Jonathan Van-Tam among others, lays out the WHO position on non-pharmaceutical interventions, NPI's, in the event of a 'flu pandemic. Isolation of sick individuals was, unsurprisingly, recommended in all cases, but contact tracing and the quarantining even of exposed individuals - let alone whole populations - were not recommended in any circumstances, as the following extract from the document's Executive Summary shows.
Please see the appendix for a more detailed outline of the UK strategy and plans.
Effective Strategic Planning Approach
Strategy
The first thing to say about an effective strategy is that it should be dynamically managed. 'Ticking the box' by creating a document which is then filed in a corner for the next ten years is most certainly not the recommended approach.
An obvious example of evolution of strategic requirements is that this pandemic has not been an outbreak of 'flu, which should have come as no great surprise to anyone given previous 'near misses' with SARS and MERS.
In addition, as far as relevant technologies are concerned, in the UK at least, the world is a far different place than it was 3, 5 or 10 years ago. Examples of 'relevant' technologies include:
Medical - vaccines (e.g. mRNA), testing (PCR, antigen, antibody), treatments, understanding of virus transmission modes (fomites, aerosol, etc.).
ICT (Information & Communications Technology) - broadband, video conferencing, data recording & reporting.
Social behaviour technologies - social media, supermarket delivery services, other.
The advances in medical technology have altered our response to respiratory disease beyond recognition since the last major pandemic (Hong Kong 'flu in 1968/9) and even since the H1N1 outbreak in 2009. Meanwhile, the widespread availability of video conferencing facilities and supermarket delivery services has enabled many of us to work from home while ordering our groceries on-line in our breaks. The use of social media as a tool for public messaging and a mechanism for public discussion needs no elaboration, other than to note the recent worrying trends regarding censorship and state propaganda.
In short, many aspects of the UK response to Covid19 would simply not have been possible ten years ago. Any strategy which is not reviewed and updated annually in order to reflect the impact of the above changes is always going to be fairly meaningless in a short space of time.
In terms of the basic approach to, and structure of, an effective overarching strategy, there are a number of key points:
A meaningful strategy must be based on a set of clearly articulated principles and objectives.
A broad strategy must cover two main areas - preparation and response.
A strategy, while high level by definition, must be real and concrete - not civil service newspeak - and must lead to real actions and measurable targets.
An example principle to underlie strategy - and arguably one that has been blown out of the water in the UK's response - is that the cure should not be worse than the disease, a variation on the medical principle of "first do no harm". Another could be to base all measures on the values of liberal democracy and a presumption of personal liberty.
Objectives might include the urgent identification and protection of vulnerable groups, minimising nosocomial infections, the avoidance of overload in the NHS, and minimising overall cost risk by spending some money up-front to save more money later - e.g. by stockpiling Personal Protective Equipment, PPE.
In terms of preparation, a usable strategy should cover a number of specific areas including:
Identification of all key stakeholders and their contributions / requirements.
The necessary focus on preventing / containing pandemics at source, through effective (globally coordinated) outbreak monitoring.
Some level of scenario planning, and associated trial exercises ('war games').
Stockpiling approach - PPE, medical assets (e.g. ventilators and testing equipment), treatments (prophylactic and therapeutic) and so on.
The professional development and testing of a general-purpose pandemic modelling tool.
Pandemic management capabilities, in particular a comprehensive data recording and analysis / management reporting tool.
The scope and approach for a detailed pandemic response plan, including a toolkit of initial actions at the start of any pandemic.
Short of actually documenting a full strategy here, some of the above items (in bold) merit a little elaboration.
Stakeholders
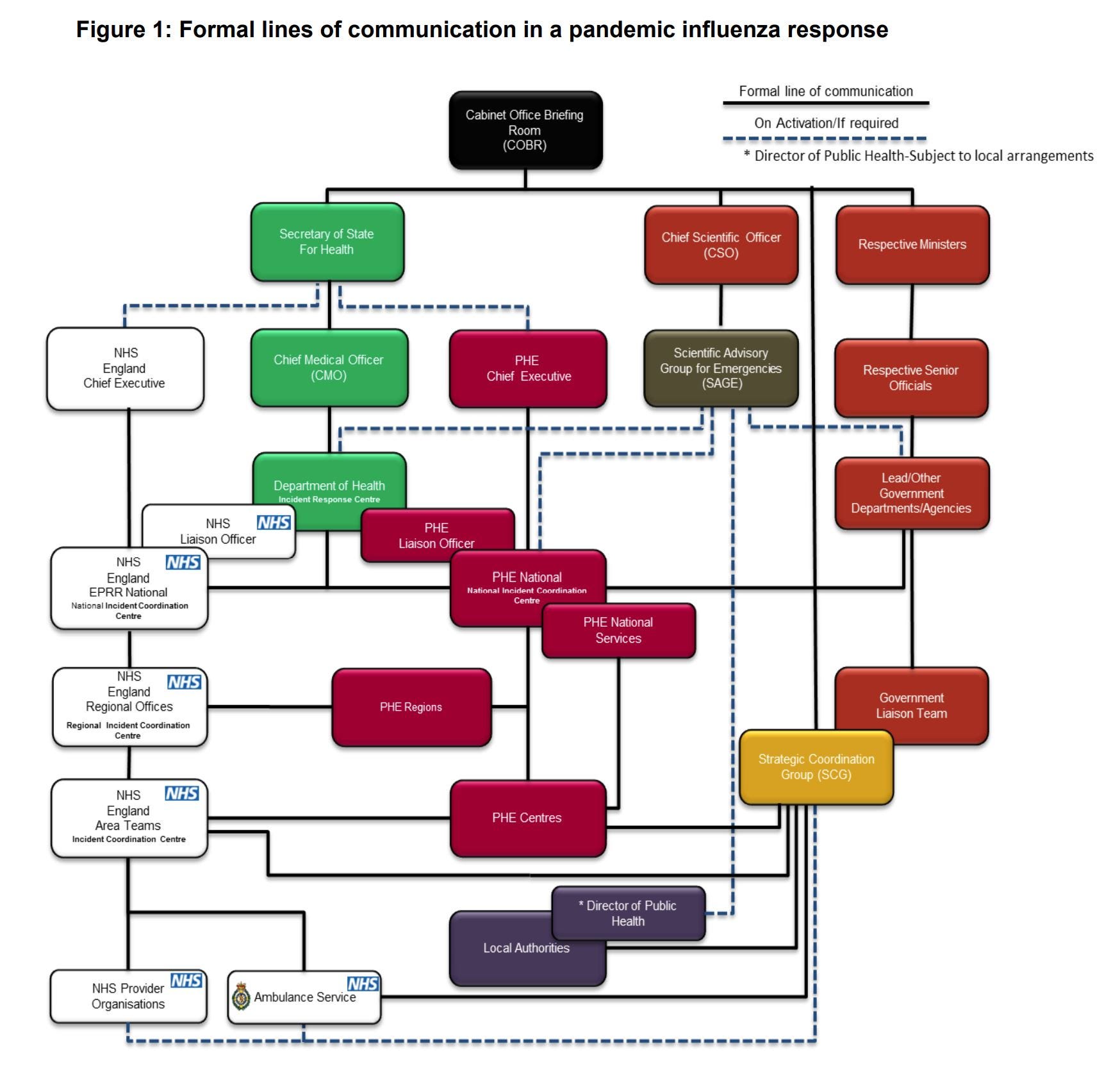
Understanding the role of all key stakeholders is fundamental to an effective strategy. Without this, there is zero chance of effectively identifying and managing all risks, issues and dependencies. In this regard, a picture speaks a thousand words and an illustration of the overall pandemic response landscape might be as follows.
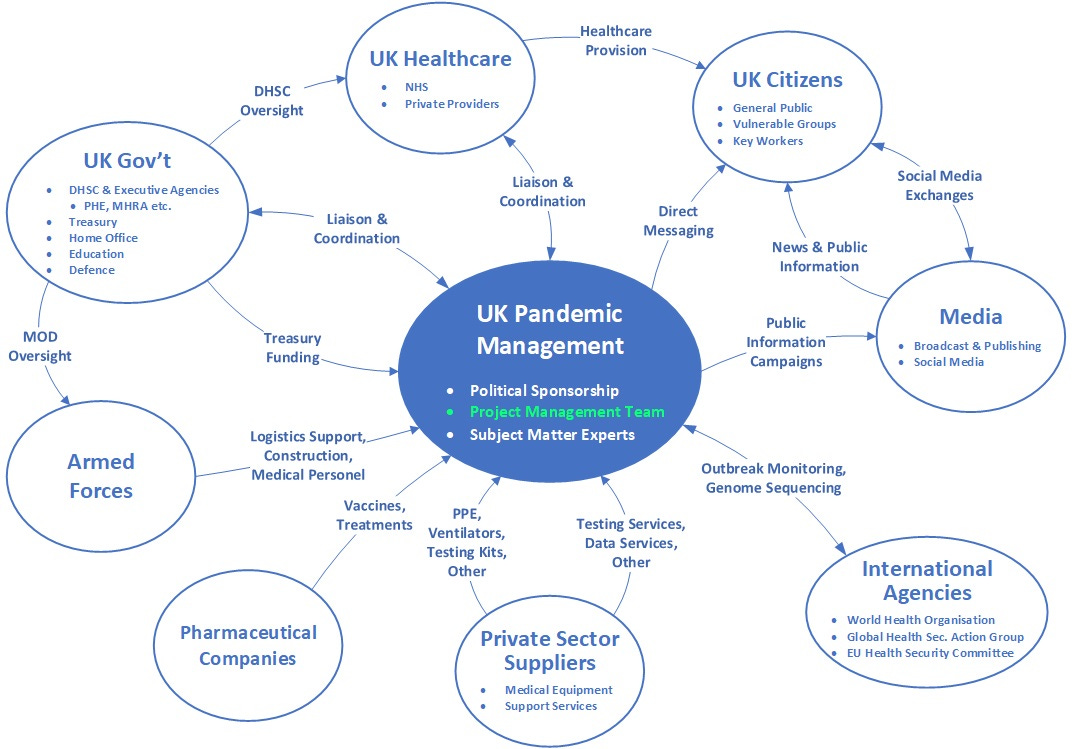
There are a number of points to stress about the above stakeholder diagram:
Firstly, there is nothing in the stakeholder landscape which could not have been clearly understood in advance and would not apply to any pandemic disease: An excuse that "we planned for 'flu" cuts no ice, especially since the DHSC strategy document referenced in the appendix explicitly mentions SARS on page 15 and elsewhere. It's a detail, and we should have planned for the general case with specific variations informed by individual 'war game' scenarios.
Secondly, the highlighted project management role/team seems not to exist - at least publicly - in the UK response. Who, other than the Prime Minister or the Health Secretary, is responsible for coordinating the overall UK pandemic response? Whatever their medical expertise, the likes of the Chief Scientific Adviser and Chief Medical Officer are not qualified for this function, yet is they and their like who are constantly wheeled out in front of our docile mainstream 'journalists' in stage-managed press conferences to explain progress.
Thirdly, the diagram is not dominated by public health specialists, epidemiologists or behavioral psychologists. There is no reason why such technical specialists should have any more prominent a role than any other subject matter experts, SME's, in a pandemic response - for example logistics experts, economists or data analysts. The role of our peerlessly professional armed forces in helping with logistics, for example, is every bit as important as input from epidemiological 'experts' who have appeared, more often than not, to have been making things up as they went along. Mask effectiveness? Cheltenham races? Transmission in schools?
Finally, there is no reference to the police as enforcers of unconstitutional civil liberties violations. The "Maintaining public order" section on page 61 of the DHSC strategy is, like the rest of the document, best ignored.
Pandemic Modelling Tool
The role of the SPI-M sub-committee of SAGE, and in particular the influence of the Imperial College modelling team, has been mired in controversy from the outset and continues to be so. The current 'cautious' plans to emerge from lockdown over several months seem to be based - once again - almost entirely on highly dubious modelling predictions.
Disregarding here the issue of whether the predictions of the "Ferguson Model" should ever have been given the prominence they got, especially given the past record of said Ferguson, the issue in focus for us is pandemic preparation. Ferguson's model was slated by many IT professionals who examined it, not because of the number of deaths it forecast but because it was undocumented, unreliable and unprofessional. A detailed review of the model is available here.
Was Ferguson's non-peer-reviewed model an appropriately professional component of a properly diligent preparation for "one of the greatest threats facing the UK"? Hardly, yet a professional review of all 'official' models, incorporating purpose, scope, design, documentation and testing would have been extremely beneficial in cost-benefit terms.
Data Management
The importance of good data, when trying to micro-manage a pandemic in the way that the UK is currently attempting, cannot be over-stated.
However, the availability of reliable data was poor initially and, while it has improved to some extent over the past 12 months, it is still far from comprehensive and consistent, and there have been some notable embarrassments along the way. Remember the 'broken spreadsheets' last October? We spent billions but were wrong-footed by an obsolete version of MS Excel.
We have at least 3 sources of official data (PHE, NHS, ONS) plus a number of 'pseudo-official' sources (such as the REACT study and the ZOE symptom tracker) which are frequently contradictory.
High quality information is either completely lacking or highly ambiguous in a number of key areas, including:
How many people in the UK have actually been exposed to the virus.
The relative rates of symptomatic, pre-symptomatic and asymptomatic spread.
The effectiveness of masks, of different types and in different settings.
The percentage of infections acquired in hospitals and care homes.
The impact of vaccine rollout on elderly mortality - 'not yet clear' more than 11 weeks after the start of vaccinations and now that all over 80's have been inoculated.
Given that the British way of life has been impacted beyond recognition in the past 12 months, and the money that has been thrown at the pandemic response, it would not be unreasonable to expect clear answers to the above questions - and dozens more - to be readily available. Instead, we are constantly treated to misleading reports from mainstream media organisations, including the BBC, often based on non-peer-reviewed pre-print studies from 'academic' institutions with partisan agendas every bit as doubtful as those of their media collaborators.
Creation of a professional data repository and reporting system is something that could, and should, have been completed in advance as part of a real and comprehensive pandemic planning exercise.
Describing a professional pandemic tracking and reporting system would require a substantial document of its own, but such a system should cover at least the following areas:
Why was such a system not built and maintained in readiness? Who can we hold accountable for this and the many other failings in our 'preparation'?
Initial Action Toolkit
The Government has been criticised in some quarters for "acting too slowly" initially. Is this true, and what should have been done more swiftly?
The accusation of dithering is generally made by those who claim that a draconian 'lockdown' should have been imposed earlier than it was. Many of these Captain Hindsight types are the very technocrats most culpable for failing to fulfil their responsibilities with adequate preparation in the first place.
Others, of course, take the view that a CCP style lockdown should never have been countenanced at all.
But there were several measures which could, and arguably should, have been implemented as soon as any risk of a pandemic was evident in early January 2020. For example, if face masks are going to be effective anywhere, one would think that crowded commuter transport systems might be a prime candidate worth at least a government advisory message.
Equally, screening of international arrivals, especially from affected areas (initially Wuhan and Hubei province) would surely have been a prudent measure from the outset - the first returnees from Wuhan were quarantined from January 31st 2020.
The main early action that seems to have been planned for was track and trace but, as we know, this quickly descended into chaos through an apparent lack of scalability (aka adequate preparation). We've persisted for months in a largely futile attempt to implement an effective track and trace system in spite of the prior WHO view that it was not feasible.
What about surge capacity in the NHS? With the help of the army (a model of professionalism as usual) we built a number of Nightingale hospitals from scratch in a few short weeks. But it seems we never had any coherent plan to staff or operate them, so they were mothballed during last summer, only for us to be told again at the start of winter that we had to re-enter lockdown to "Protect the NHS". At the very least, the Nightingales should have provided an invaluable mechanism for infection control to minimise the level of nosocomial infections during the past autumn and winter, by effective segregation of Covid and non-Covid patients. People really should be losing their jobs, if not going to prison, for professional negligence.
Plan
Unlike strategic preparation, more detailed planning can only be conducted sensibly in the context of specific scenarios from a likely range.
The only scenario appearing to influence UK planning seems to have been lessons (mis-)learned from the 2009 H1N1 outbreak - relating for example to the amount of fore-warning for the UK, the extent and severity of the disease, and the effectiveness of public communications (hence the prominent role of the SPI-B sub-committee in this pandemic).
There are a number of specific pandemic-response activities which were always likely, with varying scales depending on the exact nature of each incident - which disease, the location of the initial outbreak, the level of transmissibility and so on. Such general activities are sector-specific and an effective response would need a set of coordinated plans to address each area. The list of considerations is long but would include, for example:
Identification and protection of vulnerable groups.
Enhanced infection control measures in hospitals, including effective segregation of those known to be infectious.
Mitigation of any school closure measures, e.g. staggered classes, exceptions for key worker families, remote learning arrangements etc.
Management of risk on public transport, especially crowded commuter services.
Airport facilities for screening international arrivals.
Fast-tracking the development & approval of therapeutic and prophylactic treatments, vaccines and so on.
Logistics for distribution of treatments and tests - for example Vitamin D supplements for care home residents and the establishment of local testing centres as necessary - as well as arrangements for effective track and trace operations.
Compensatory payment arrangements for people affected by mitigation measures - for example those asked to self-isolate.
Data tracking and reporting arrangements.
Aside from the specific subject areas which should be covered in detailed plans, there are a number of very well understood specific purposes of programme and project plans in general, including:
Scope and objectives.
Organisation structure, with clearly articulated roles and responsibilities.
Risk tracking.
Budgeting and cost tracking.
Governance and reporting mechanisms.
Far more could be said here about an effective process for detailed planning. Suffice to say, if such a document set exists in the UK it has been a very well-kept secret.
In light of the failure of our bureaucratic class to prepare effectively, the success that the UK has had in some areas - for example the building of the Nightingales, the identification of dexamethasone and other treatments, the rapid development and approval of the Oxford Astra Zeneca vaccine, the expertise in genome tracking - have been all the more remarkable. Such successes have been achieved in spite of, not because of, effective pandemic planning and they have mostly come in areas where the UK has substantial pre-existing expertise - particularly in the life sciences sector.
The Negative Impact of Poor Preparation on Real-time Response
Let's first summarise the key factual results of the UK's pandemic response - as far as it is possible to objectively establish the facts, given the issues of data transparency which persist to this day.
Cumulatively, 120,000 'Covid related' deaths across the UK (PHE)
Compared to 5 year average death rates, 107,000 excess deaths in England and Wales since the start of 2020: 75,000 in 2020, plus 32,000 in the first 6 weeks of 2021 (Office for National Statistics, ONS)
Up to 30% of infections for all hospital 'Covid admissions' acquired in hospital.
Of the 54k excess deaths to 12th June 2020 in England and Wales, 19k (35%) are attributable to 'Covid related' deaths in care homes between 2 March and 12 June 2020. If we posit that 30% (9k) of the 28k 'Covid related' hospital deaths in England to 12 June 2020 resulted from hospital-acquired infections, we get to a total of 19 + 9 = 28k. That's 28k potentially avoidable deaths, with more effective infection control measures in critical settings, in the first 3 months alone; 52% of the 'Covid related' total in England & Wales for the period.
A full year of disrupted education in schools and universities. And counting. Secondary school children possibly required to wear face masks in class until at least Easter and subjected to frequent repeat testing. Exams cancelled for the second year in succession.
Disregarding Gibraltar and San Marino, the fourth highest death rate per 100,000 population in the world, according to the WHO.
The worst economic impact in 300 years. Ongoing.
The most extreme reversal of civil liberties and fundamental rights since King John was 'persuaded' to accept the Magna Carta.
Tens of £ Billions spent inefficiently - and possibly illegally - on PPE contracts, ineffective track and trace systems, unused Nightingale hospitals and so on.
In the interests of balance, we must recognise that the development, procurement and rollout of vaccinations appears to be a great success story so far.
We suggest that the panicked initial reaction - and every part of the subsequent chaotic response - to the crisis in the UK was largely due to the failure to adequately prepare.
In reviewing the negative impacts, there is one key point to emphasise above all else: The people and organisations who failed to adequately prepare, while repeatedly regurgitating the mantra that a pandemic was one of the top threats to national security, are the very same people that we have entrusted to manage the response. Democratically elected politicians have mostly been side-lined, and have attempted to abrogate themselves of all responsibility for our descent into a totalitarian catastrophe.
Authority has been ceded to unelected technocrats led by SAGE, the Chief Medical Officer, CMO, and the Chief Scientific Adviser, CSA. But who accepts accountability for the disastrous outcomes listed above?
The unhealthy symbiotic nature of the relationships between key parties involved in the response has been a critical compounding factor in a story dominated by bureaucratic navel-gazing and group-think. A cosy club of government agencies such as Public Health England, 'big pharma' interests, academic institutions such as Imperial College, and left-liberal establishment journalists, has not served the public well during this crisis.
Others have speculated on the motivations behind some of the funding arrangements, given the financial relationships between globalist 'philanthropists', UN agencies, state actors such as the Chinese Communist Party, CCP, and individuals / institutions directly involved in the pandemic response in the UK and elsewhere.
Conclusions
In this paper we have reviewed the UK preparations for a pandemic, but it is the response and its impact on the country which is most important in the final analysis.
In common with much of Europe and many US States, the results of the UK's response have been catastrophic and, in terms of the socio-economic impact, the cure has undoubtedly been worse than the disease.
We examine the consequences in a number of areas below.
Democratic Rights and Freedoms
In spite of the UK having been transformed into a totalitarian state, our sickness and death rates have been among the highest in the world. Sweden and others achieved better public health results, by following the science and without resorting to authoritarian lockdowns.
Democracy in the UK has sunk very low indeed when the only place to protest legally against lockdown is in the (largely virtual) House of Commons. We now compare unfavourably with the likes of Belarus, Russia and China - which ought (but seems not) to give serious pause for thought to our government.
Our freedoms have been abolished or diminished to such a degree that idea of the UK as a bastion of democratic rights and freedoms for the British people is now but a wild myth. We have watched the Government systematically curtail civil liberties, and the Metropolitan police brutally attack and detain people, including lone women, for daring to protest the lockdowns - ref. the Subject Access youtube channel. All the while being cheered on by the Home Secretary threatening ever-increasing totalitarian measures against all dissent, the irony of her stance lost on her.
Having set the worst of precedents, how easy it would now be, armed with such a blueprint of oppression, to implement another Marxist lockdown in response to any real or perceived national threat.
All this as a reaction to a horrible, but by no means historically unique or exceptional, pandemic - comparable perhaps to the Hong Kong ‘flu outbreak of 1968 which claimed up to 4 million lives globally.
Is this the United Kingdom we really want to live in? The loss of this great country ‘on our watch’ should instill an overwhelming sense of shame in all right-thinking people. What legacy does the trampling of these rights over the past 12 months leave us; how can we ever regain our precious democratic freedoms and fundamental human rights?
Pandemic Approach and Methodology
The UK did not ‘follow the science’, instead we ignored and discarded it. The previous rule book for pandemic response, as articulated by the WHO and public health authorities in all free democracies, has been shredded on the flimsiest of evidence.
In the absence of a sound planning baseline, we had no solid strategic foundation on which to judge events or to construct a cool-headed, truly evidence-based, response. Our response was instead 'informed' by highly dubious propaganda emanating from communist China, whose obfuscation and deceit has wrecked western societies and economies while leaving China itself relatively unscathed. Rather than implementing a pre-planned set of effective actions based on a comprehensive pre-existing strategy and a solid foundation of preparation (because these things did not exist), the government responded to hysteria propagated by sensationalist media reports from Lombardy and 'leaked' videos from China of officials in hazmat suits and members of the public collapsing theatrically in the streets.
Following the initial panic, and again in common with many other countries such as Ireland and the US, the UK response has been dictated by a small group of unelected, extremist 'public health' zealots who have demanded ever more draconian measures - the latest likely to include mandatory wearing of face masks for all secondary school students and vaccine passports - in order to 'control a virus' which we have very manifestly failed to control where it most mattered; in hospitals and long term care facilities. Up to half of UK Covid related deaths may have been avoidable with better infection control measures in these settings.
Those of us who, prior to last year, never gave much thought to the risk of devastating health and socio-economic impacts from a global pandemic, might now be accused of 20:20 hindsight, but it was never our job to develop a strategy and plan for "one of the highest risks faced by the UK". It was however the job of the public health specialists, and others, who were and are well-compensated to do exactly that. It is not unreasonable to question whether our civil service mandarins were asleep on the job, and to ask why we are still trusting these same people, led by the Chief Medical Officer and Chief Scientific Adviser, to get us out of this mess.
In the arena of pandemic planning and management, many thousands if not millions of lives are at stake. The UK has failed to adequately protect its vulnerable population, the economy has taken an unprecedented battering, our youth have borne the brunt of a disrupted education, and civil freedoms hard-won by generations of our ancestors have been lost, probably permanently.
In denouncing the behaviour of our own 'public health experts', we should not forget the leading role of the WHO in the shambles of the initial global response. In their recent visit to Wuhan, they've ably demonstrated a complete inability to learn the error of their ways.
Our mainstream media is also culpable. Part of their role, as they never tire of telling us when it suits their agenda, is to 'speak truth to power' and to hold those in authority responsible for their (in)actions. Instead, they have gleefully jumped on the psy-ops bandwagon, actively collaborating in the governments disgraceful campaign to gaslight the nation.
We now see the beginnings of a new narrative, pushed by many of the same people who have overseen the decimation of the UK. Led by our Prime Minister, together with the unelected globalists behind the scenes - the likes of Prince Charles, Tony Blair, and their international counterparts such as Gates, Schwab and many other usual suspects - the agenda is now shifting inexorably to the global ‘Climate Emergency’.
A Road Map to Hell
All indicators now show the disease to be waning fast and, in typical seasonal fashion, likely to ‘disappear’ entirely with the imminent arrival of Spring. Yet we are to be subjected to several more months of ridiculous lockdown rules with no credible evidence to support their necessity.
We can now expect a concerted attempt to continue key restrictions, in particular international travel and general consumer freedoms such as meat consumption, to 'save the planet'. Next week's budget will merit close scrutiny as far as any imposition of "green taxes" is concerned; watch this space.
In the short term, the Prime Minister's hopelessly inadequate 'road map' leaves us no wiser as to when this fiasco will be over and - other than the incoherent 'Build Back Better' mantra - what happens next, or how we repay the accumulated debt of the past 12 months.
Summary of Results
Any dispassionate, objective assessment of the outcomes - away from the metropolitan left-liberal echo-chamber inhabited by our politicians, mainstream media and public health establishment - must conclude that the outcome for the UK has been woeful.
Before 2020, subjecting an entire population of healthy people to house arrest would rightly have been considered as totalitarian abuse of human rights.
In spite of extreme lockdown measures, UK death rates have been among the highest in the world. The damage in terms of ‘collateral’ illness and deaths (cardio-vascular disease, cancer, mental health, suicides and so on) is as yet unknown.
Far from ‘following the science’, the burden of proof has been shifted from the lockdown fanatics needing to demonstrate benefits, to the 'sceptics' having to prove their ineffectiveness. Proving a negative is usually impossible, but fortunately we have real-world evidence - from Sweden and elsewhere - to indicate that lockdowns do not improve outcomes.
We quickly discarded all previous scientific knowledge and instead based our response on hysteria fomented by CCP propaganda and home-grown activists driven by political and financial incentives rather than the national interest.
Covid19 will now be with us as an endemic seasonal (winter) virus. Yet the government shows no desire to expedite the end of lockdown. They have instead done the opposite and unnecessarily extended the agony for many months yet.
If, as a nation, we do not urgently learn the lessons of the past year’s failings, we can ‘look forward’ to more destructive, unnecessary lockdowns next winter - when the NHS inevitably comes under pressure once again, as it has done every winter in living memory.
The trampling of human rights over the past 12 months leaves us with a dangerous legacy, as the same ‘elite’ factions inevitably now turn their focus to climate change.
Road to Recovery
We now need an urgent public enquiry, not one that provides an excuse to kick the ball into touch for the next three years, with preliminary findings published within 3 or 4 months. We must do whatever is necessary to prepare the NHS for the inevitable pressures it will face next winter - pandemic or no pandemic. This does not mean throwing money indiscriminately at poorly articulated issues, but a professional external - and truly independent - review of NHS surge and contingency planning, with defined roles for our armed services where necessary.
In searching for a chairperson for the much-needed enquiry, we would do well to start with the likes of Lord Sumption.
Finally, the guilty must be held accountable for their failings and they must be replaced with professional experts who are not compromised by links to big pharma, globalist finance or far-left political agendas.
Appendix - Details of UK Pandemic Planning Preparations
There are a number of official documents addressing various aspects of pandemic planning and response.
The UK Influenza Pandemic Preparedness Strategy 2011 is the overarching document from the Department of Health and Social Care, DHSC, while the related Health and Social Care Influenza Pandemic Preparedness and Response, produced in 2012, "focuses predominantly on the operational aspects of pandemic response in the health and social care sectors".
The key Public Health England, PHE, documents - 'Pandemic Influenza Strategic Framework' and 'Pandemic Influenza Response Plan' - are from 2014 and are available on the UK Government web portal here.
UK Influenza Pandemic Preparedness Strategy
A review of the DHSC document doesn't start promisingly. The target audience reveals it to be an internal health sector document, while the description claims it to be "the Government's strategic approach".
There is no clarity on how the document was produced, who contributed specialist input, any detailed relationship with other documents in a coherent set (the 'Further Information' at chapter 8 is all but worthless) and so on. Selected quotes from the introduction are listed below (emphasis added).
Paragraph 1.3:
"a new influenza pandemic continues to be recognised as one of the greatest threats facing the UK"
Paragraph 1.5:
"Prepare for an influenza pandemic that may have a high impact on the health system and wider society"
Paragraph 1.10:
"Take better account of the learning from behavioural scientists about how people are likely to think, feel and behave during an influenza pandemic"
Paragraph 1.11
"This strategy has been developed jointly across the four UK Governments, with professional, NHS, social care and public health organisations, and based on advice from clinical, scientific and other experts"
Suddenly on page 12 of the document, seemingly apropos of nothing, we get a comment on the potential economic impact of a pandemic:
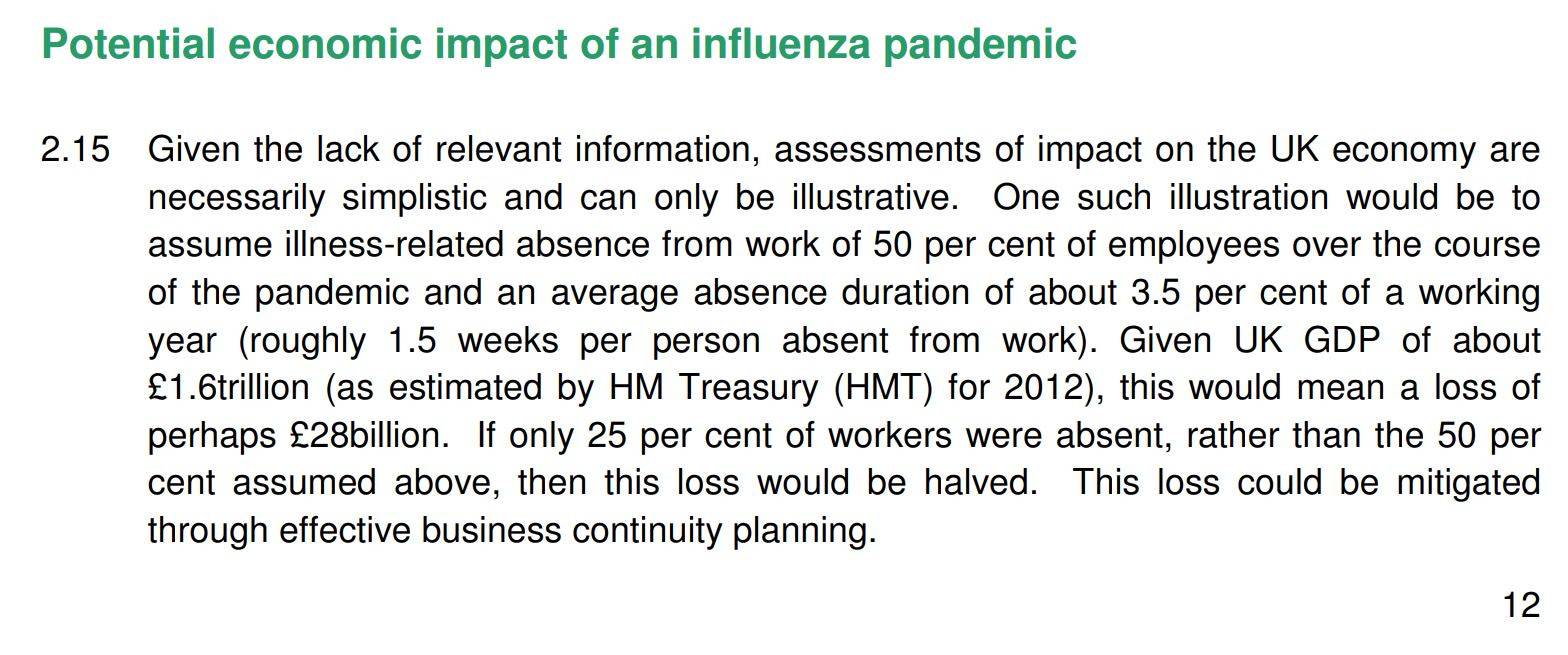
The document does not improve as one reads further. On pages 21 & 39/40 it mentions possible school closures, but provides no analysis or suggestions about how to limit or mitigate any effects, nor any links to more detailed or departmental (e.g. department for education) documents that might address this issue. Universities aren't mentioned other than, on page 59, this: "Universities and Colleges all have their own business continuity plans and will make their own decisions on closures or partial closures based on advice from public health services". On page 26, the document briefly dismisses the usefulness of WHO messaging in the 2009 H1N1 "pandemic", but doesn't seriously address the hopeless inadequacy of the WHO as the ineffective bureaucracy it has proven itself to be over the past 12 months. On page 26, the public use of face masks is discussed in vague terms, "research" is quoted which is not referenced, and so it goes on.
Tellingly, and tragically, chapter 6 - The health and social care response - makes no specific mention of care homes, nor of general infection control measures in hospital or residential care settings.
Finally, there is a Glossary of Terms of a sort at the end of the document, in the Acronyms section. Conspicuous by their absence in this section are definitions of some critical terms which have been quoted with abandon over the past 12 months. What is a 'Case'? An 'Infection'? What do we mean when we talk about 'Immunity'? (Vaccine-derived) herd immunity is referenced briefly in a footnote on page 44, that's about it.
As they say on social media these days, the entire document is word salad.
The second DHSC document referenced above, "Health and Social Care Influenza Pandemic Preparedness and Response", is similarly an 'interesting read' but not useful in terms of any content for practically preparing for and responding to a pandemic emergency.
Perhaps PHE fared better?
PHE Documents
The foreword of the PHE Strategic Framework includes the following statement, mirroring the claim of the DHSC that we all take the risk of a pandemic very seriously.
"The prospect of a flu pandemic is one of the highest risks faced by the UK"
This was clearly always true and it remains devastatingly so today with the bitter experience of the past 12 months, albeit that the culprit was Covid19 rather than the 'flu.
The first thing that jumps out from the Strategic Framework is that it isn't very "strategic". Frankly, more of a navel-gazing exercise by PHE. We should not blame PHE for a lack of strategic thinking, as they aren't really set up for that, but we can and should criticise them for the general lack of professionalism shown in the document: It's mostly waffle, references related documents for no obvious reason (no clarity as to how the documents relate to each other as a coherent set) and with no quality assurance, QA, details (version numbers, dates etc.).
In the PHE Strategic Framework, as with the DHSC documents, there isn't a single diagram, no recognition of external stakeholders (i.e. outside of PHE), there are internal inconsistencies (the foreword says "This strategic plan", but the document title is "Pandemic Influenza Strategic Framework"). And so it goes on. For a document purporting to address "one of the highest risks faced by the UK", it is not impressive.
Maybe the detailed plan provides a more useful basis for an effective response? As ever, we are sternly reminded of the severity of the threat. From the Executive Summary on page 6:
"The threat from pandemic influenza remains the top national risk"
Also in the Scope section on page 10:
"Given the uncertainty and the potential impact of influenza pandemic, pandemic influenza has been classified by the Cabinet Office as the number one threat to the UK population"
Aside from the question of whether anyone ever proof-read the document for the use of coherent English, how many times do we need this peculiarly bureaucratic style of virtue-signalling piety to understand that the threat of a pandemic is 'serious'?
This particular document is longer than the others, at 88 pages including appendices. For the first time, on pages 19 & 21, we have a couple of diagrams; organisation charts of sorts, although quite what their purpose is in this context remains unclear.

The rest of the PHE plan continues in the same vein as the rest of the document set. Further analysis is futile. In short, the entirety of the strategic planning documentation is a poorly conducted exercise in bureaucratic shuffling of deckchairs.